
Saphenion®: Venenkleber bei aneurysmatischen Krampfadern
Saphenion®: Vein glue therapy of aneurysmatic veins
Saphenion®: Venenkleber bei aneurysmatischen Krampfadern – Der Venenkleber Venaseal® hat die uneingeschränkte Zulassung für die Therapie von Stammkrampfadern. Unabhängig davon kann der Kleber auch erfolgreich bei der Therapie von Seitenastkrampfadern, Perforansvenen und Aneurysmata der Venen mit Erfolg im Rahmen des „off label use“ eingesetzt werden.
Die Therapie von stark erweiterten Krampfadern (Aneurysma) stellt sich für alle bisher bekannten Therapieverfahren als zusätzlich schwierig und komplikationsreich dar. Bei der radikalen „Stripping“ – Op besteht ein sehr hohes Risiko eines Einrisses der weichen und erheblich unter Spannung stehenden Venenwand. Die Folge sind massive Blutungen und eine nicht vollständige Entfernung der defekten Vene. Ausserdem sind große Hautschnitte zur Freilegung der Krampfadern notwendig, um ein möglichst umfassendes Bild von der Gewebesituation zu bekommen.
Die Katheterverfahren, insbesondere die seit 21 Jahren im Einsatz befindlichen thermischen Verfahren Laser und Radiowelle, können mittels hoher thermischer Energieabgabe ebenfalls bei der Behandlung von erweiterten Krampfadern eingesetzt werden. Allerdings ist die notwendige Energiemenge (Hitze) dafür deutlich höher, so daß auch das Risikio für thermische Gefäß-und Gewebeschäden (Nervenläsionen, Lymphbahn-/ Lympfknotenverletzungen!) wesentlich erhöht ist.
Bei den nicht thermischen Verfahren Mikroschaum, Venablock® und ClariVein® ist ein effektiver Einsatz an stark erweiterten Krampfadern und an Krampfaderaneurysmen sehr fraglich, wenn nicht kontraindiziert. Einzig mit dem Venenkleber- System VenaSeal® ist nach unseren Erfahrungen eine effektive – und gleichzeitig nebenwirkungsarme Therapie der Aneurysmavenen möglich und sinnvoll.
Super glue VenaSeal® has the approval for therapy of greater truncal veins. Independently of this super glue can be used also in the ablation of side branches, perforator veins and aneurysmatic veins. this is a successful „off label use“.
The therapy of strongly dilated varicose veins (aneurysms) is also difficult and complex for all previously known therapy methods. In the radical „stripping“ operation there is a very high risk of tearing the soft vein wall that is under considerable tension. The result is massive bleeding and incomplete removal of the defective vein. In addition, large skin incisions are necessary to expose the varicose veins in order to get the most comprehensive picture possible of the tissue situation.
The catheter procedures, in particular the thermal procedures laser and radio wave, which have been in use for 21 years, can also be used in the treatment of enlarged varicose veins by means of high thermal energy output. However, the amount of energy (heat) required for this is significantly higher, so that the risk of the thermal vessel and tissue damage (nerve lesions!) Is also significantly increased.
With the non-thermal methods of microfoam, Venablock® and ClariVein®, effective use on greatly enlarged varicose veins and varicose vein aneurysms are very questionable, if not contraindicated. According to our experience, only the VenaSeal® vein glue system is an effective therapy of the aneurysm veins, with few side effects, possible and sensible.
Saphenion®: Venenkleber bei aneurysmatischen Krampfadern – Fallbeispiele
Saphenion®: Vein glue therapy of aneurysmatic veins – some cases
Saphenion®: Venenkleber bei aneurysmatischen Krampfadern – aneurysmatischen Fussrückenvene
Wir behandelten einen Patienten mit einem postthrombotischen Syndrom des li. Beines mit gleichzeitiger primärer und sekundärer Stamm – / Seitenastvaricosis dieses Beines und einer primären Stammvaricosis am re. Bein. Hier fand sich auch ein kleinapfelgrosses Aneurysma einer Fussrückenvene (Bilder oben). Wir behandelten beide Stammvenen der Saphena magna simultan mittels VenaSeal – Venenkleber. Dnach verklebten wir das Aneurysma des re. Fussrückens. Wir injizierten 3 Tropfen Kleber (=0,27ml) in diese spezielle lokale Venenveränderung.
Saphenion®: Vein glue therapy of aneurysmatic veins – aneurysmatic dorsal venous arch
Today we treated one patient with a post-thrombotic syndrome of the left leg in relation a varicose greater saphenous vein and a lot of side branches. On the right side, we also found a varicose greater saphenous vein and the aneurysmatic vein of the dorsal venous arch. We treated the truncal veins of both legs simultaneously with VenaSeal®. After this, we ablated the aneurysmatic vein of the right foot also with super glue. We used 0,27 ml (3 drops) of glue for this special local situation.

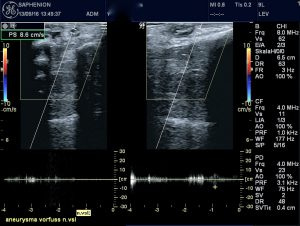
Die Therapie des Vorfußaneurysmas mit dem Kleber erfolgte off label. Wir entschieden uns im diesem Fall anstatt einer Mikroschaumtherapie zur Anwendung des Klebers auf Grund des Durchmessers und der Länge des Aneurysmas. Nach der Behandlung sahen wir einen normalen Befund ohne Hautschnitt oder andere Verletzungen (Bilder unten).
The aneurysmatic tumour of the right foot was treated off label, We decided to use glue instead of using microfoam because of the great diameter and length of this aneurysmatic vein. At the end of the day, we saw a normal clinical diagnosis without any cut.


Saphenion®: Venenkleber bei aneurysmatischen Krampfadern – 12 Monate nach VenaSeal
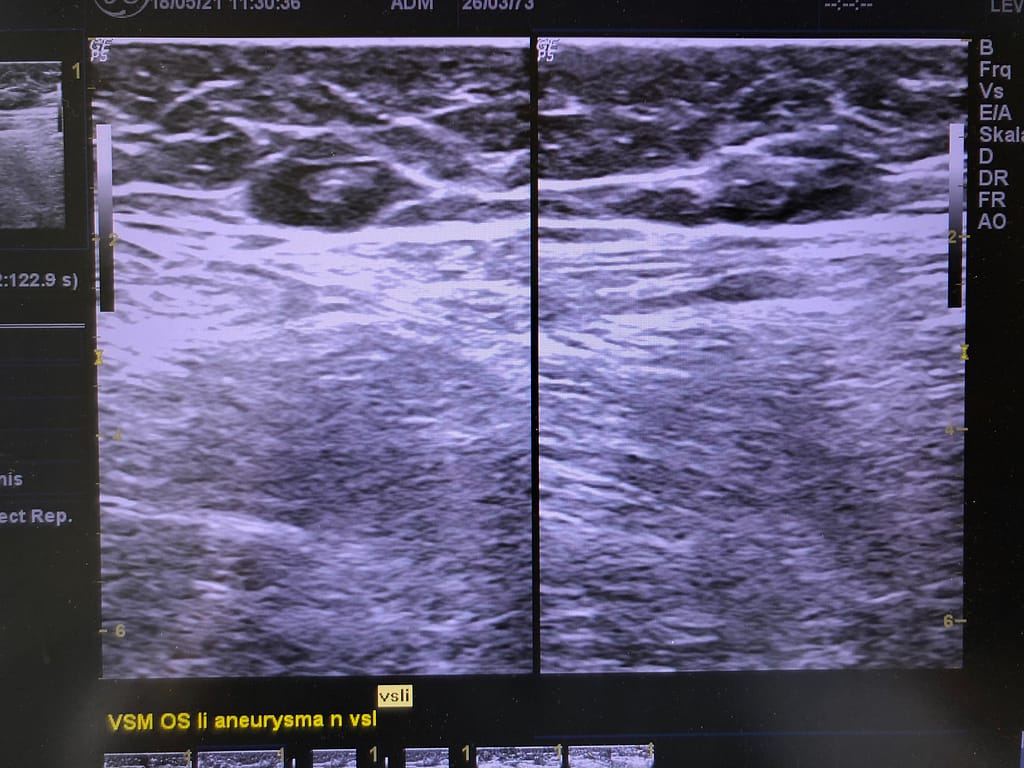
Die Nachuntersuchung 12 Monate nach der Therapie mit VenaSeal ergab einen unauffälligen klinischen und monografischen Befund sowohl der ektatischen Stammvene Saphena magna, als auch des behandelten Fussrückenaneurysmas – dieses war klinisch visuell und palpatorisch nicht mehr sichtbar.
Saphenion®: Vein glue therapy of aneurysmatic veins – clinical and ultrasound control after 12 months
The post-operative control examination 12 months after VenaSeal therapy was clinically, sonographically and upon palpation unnoticeable. The ecstatic GSV was effective closed and the aneurysmatic vein at the instep was not to see or papable.


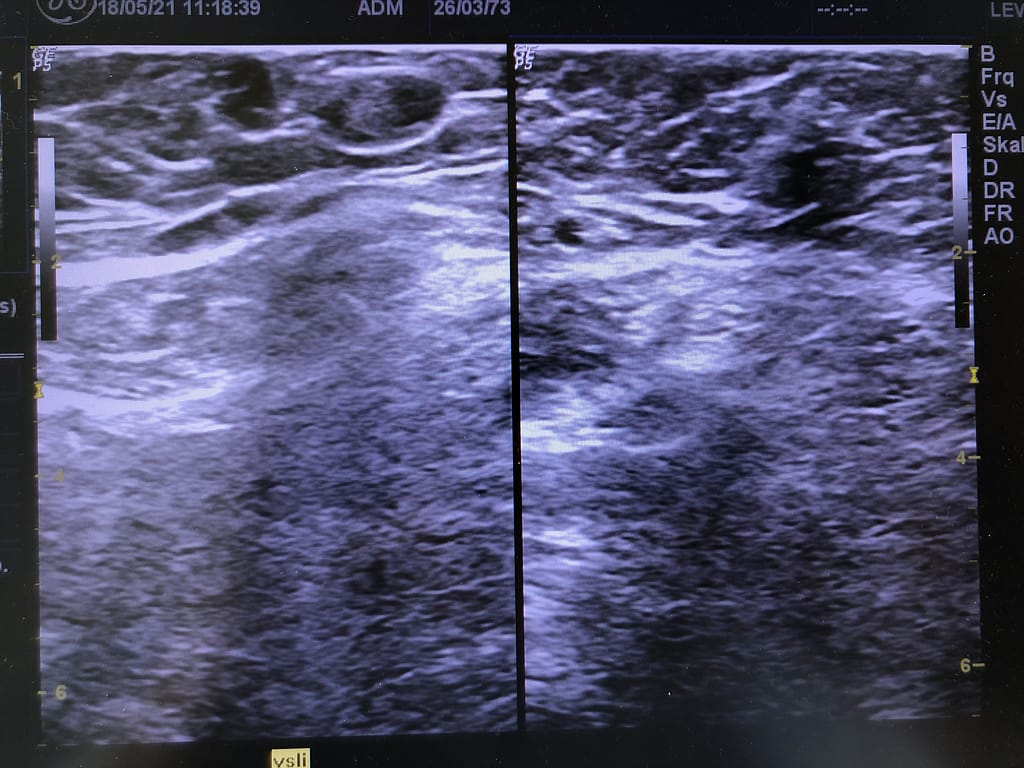
Saphenion®: Venenkleber bei aneurysmatischen Krampfadern – Magna-Aneurysma
Eine andere Therapie erfolgte an beiden Magnastammvenen. Die rechte Vene war mit einem Durchmesser von 0.6 – 0,8 cm typisch erweitert, die li. Saphena magna hatte über einen längeren Venenabschnitt am Oberschenkel einen Durchmesser von 1,8 – 2,3 cm. Das rechte Bein wurde entsprechend des Therapieprotokolls behandelt. Am li. Bein wurde die Therapietechnik leicht abgewandelt. Wir injizierten hier alle 2 cm einen Tropfen 0,09 ml Kleber entlang des Aneurysmas – sehr wichtig ist in diesem Fall die Lagerung des Patienten. Eine strikte Trendelenburg – Lagerung ist sehr wichtig. So konnte auch in diesem Fall ein ausgezeichnetes Ergebnis des Venenverschlusses erzielt werden.
Die Therapie des Aneurysmas der V. saphena magna li. mittels Venenkleber war ebenso erfolgreich. Der Venendruck konnte durch die Verklebung der Stammkrampfadern bereits unmittelbar normalisiert werden, das Aneurysma war komplett verschwunden.
Saphenion®: Vein glue therapy of aneurysmatic veins – aneurysm of GSV along the tight
Another therapy was a varicose GSV on both legs, the right side the diameter was 0,6-0,8 cm, we treated related to the technical protocol. The left GSV was dilated with a maximal diameter of 2,3 cm like an aneurysm. We treated with the same catheter in an adapted technique – a drop of glue every 2 cm along the aneurysm – very important in this case is the position of the patient. It`s very important, to make a Trendelenburg position. So the results in sealing aneurysm veins are amazing!
The treatment of the GSV aneurysm was also effective along whole the treated vein – You can see it on the ultrasound pictures. The post-op vein pressure of the legs was normalized by VenaSeal – ablation of insufficient greater saphenous veins, the local aneurysm was missing completely.


Saphenion®: Venenkleber bei aneurysmatischen Krampfadern – Das Mündungsaneurysma
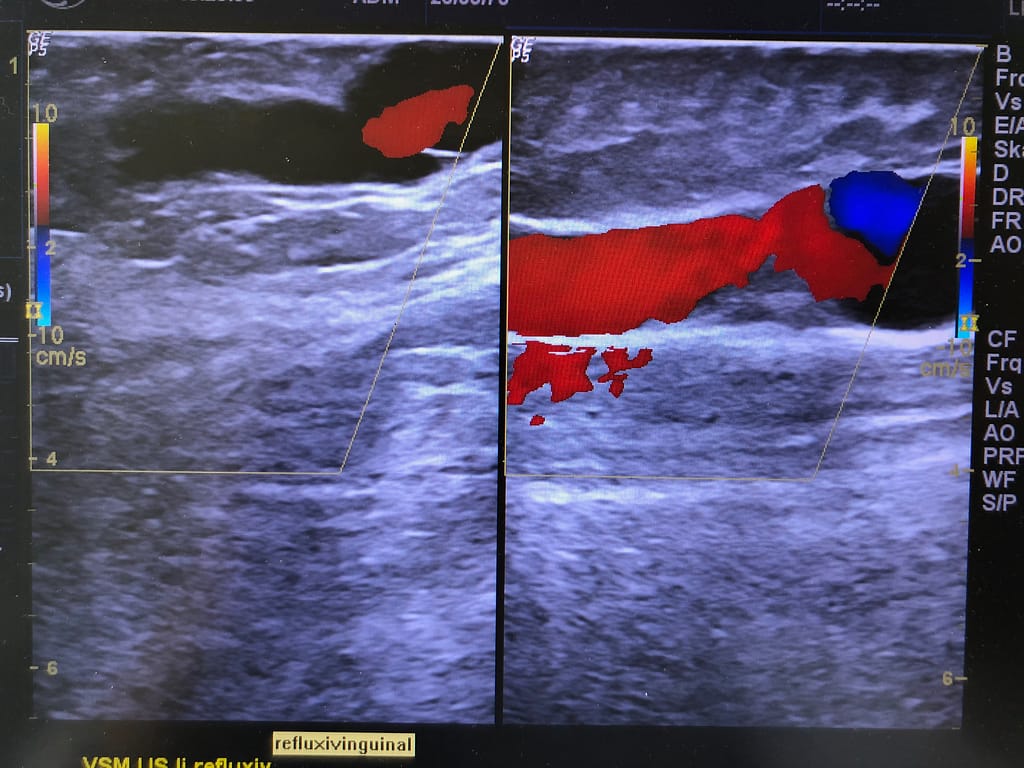
Gar nicht selten sehen die Gefäßchirurgen und Venenspezialisten im Ultraschall massive aneurysmatische Aufweitungen der Stammveneneinmündungen ( Magna-/ Parvacrosse). Zum Einen anlagebedingt, zum Anderen ist eine der Ursachen die Anzahl der einmündenden Seitenastkrampfadern. Diese kommen vom Bein, aber auch aus dem Schambereich und den Bauchdeckenvenen.
Wie in den unten sichtbaren Ultraschallbildern auch vom nicht Erfahrenen zu vermuten, sind die Strömungsverhältnisse in diesen Mündungsaneurysmen erheblich gestört. Nicht nur der Rückfluß des venösen Blutes in die Beinvenen ist sichtbar, auch eine Verwirbelung des Blutflusses in alle Richtungen kann im Ultraschall dargestellt werden. Die Therapie dieser monströsen Gefäßveränderungen stellt jeden Operateur, egal ob er klassisch operiert oder mittels der verschiedenen Katheterverfahren therapiert, vor einige Sorgenfalten. Das liegt zum Einen an der hohen Verletzungsgefahr dieser Venen, zum Anderen an den methodenspezifischen Grenzen der verschiedenen OP-Verfahren.
Saphenion®: Vein glue for aneurysmal varicose veins – the junction aneurysm
It is not uncommon for vascular surgeons and vein specialists to see a massive aneurysmal widening of the truncal vein junctions (GSV / SSV) in the ultrasound. On the one hand due to the condition, on the other hand, one of the causes is the number of confluent lateral varicose veins. These come from the leg, but also from the pubic area and the abdominal wall veins.
As can be assumed by the inexperienced in the ultrasound images visible below, the flow conditions in these estuary aneurysms are considerably disturbed. Not only the backflow of the venous blood into the leg veins is visible, but the turbulence of the blood flow in all directions can also be shown in the ultrasound. The therapy of these monstrous vascular changes puts every surgeon, regardless of whether he operates conventionally or uses the various catheter procedures, with some worry lines. On the one hand, this is due to the high risk of injury to these veins and, on the other hand, the method-specific limits of the various surgical or catheter procedures.


Die erfolgreiche Therapie mittels VenaSeal® – Venenkleber wurde durch einige Modifikationen der Kathetertechnik möglich. Zunächst wurde der Katheter bis 2 cm an die Einmündung hergeschoben. Dann erfolgte eine Kopftieflage des Patienten (Trendelenburg-Lagerung). Zunächst wurde ultraschallgesteuert das Aneurysma verklebt, hierbei ABgabe von Klebertropfen jeden Zentimeter und manuelle Verteilung des Klebers auf der Gefäßwand. Die Mündung in das tiefe Venensystem wurde nicht mit dem Ultraschallkopf abgedrückt, hier führten Zeige – und Mittelfinger den Druckverschluß der Einmündung durch. Nach einer Kompressionszeit von 2 Minuten wurden dann mittels Ultraschall das Aneurysma überprüft. Nicht verklebte Abschnitte wurden dann mittels isolierter lokaler Punktion und Injektion von 2-3 zusätzlichen Klebertropfen erfolgreich verklebt.
The successful therapy with VenaSeal® – vein glue was made possible by some modifications of the catheter technique. First, the catheter was pushed up to 2 cm from the junction. The patient was then placed in a head-down position (Trendelenburg position). First of all, the aneurysm was glued under ultrasound control, dispensing drops of glue every centimetre and manually distributing the glue on the vessel wall. The junction into the deep vein system was not pressed with the ultrasound head, here the index and middle fingers performed the pressure lock of the opening. After a compression time of 2 minutes, the aneurysm was then checked by means of ultrasound. Non-glued sections were then successfully glued by means of isolated local puncture and the injection of 2-3 additional drops of glue. An ethanol compression bandage was then applied immediately.


Saphenion®: Venenkleber bei aneurysmatischen Krampfadern – Aneurysma von Krampfadergabelungen
Als ein weiteres Beispiel für die gute Effektivität nach der Therapie mit dem nicht thermischen Verfahren des Venenklebens möchten wir abschließend ein Venengabelaneurysma darstellen. Es handelt sich hierbei um eine Vena saphena magna am Oberschenkel und den Abgang einer akzessorischen Stammkrampfader. Hier wurde die Vena saphena magna in typischer Weise behandelt, einschließlich der bekannten Kopftieflagerung nach Trendelenburg, Unter Ultraschallsicht wurde dann die Venengabel dargestellt.
Oberhalb der Venengabel, direkt am Abgang der akzessorischen Vene und unterhalb der Gabel wurde jeweils ein zusätzlicher Klebertropfen injiziert. Diese wurden dann mittels Fingermassage über 10-15 Sekunden im Bereich der Venengabel und auch in die einmündende akzessorische Stammvene hinein massiert. Anschließend erfolgte auch hier das sofortige Anlegen eines Kompressionsverbandes
Saphenion®: Vein glue for aneurysmal varicose veins – aneurysm of varicose vein bifurcations
As a further example of the good effectiveness after therapy with the non-thermal method of venous gluing, we would like to conclude with a venous bifurcation aneurysm. This is a great saphenous vein on the thigh and the exit of an accessory trunk varicose vein. Here the great saphenous vein was treated in a typical manner, including the well-known Trendelenburg head-down position. The vein bifurcation was then shown under ultrasound view.
An additional drop of glue was injected above the vein bifurcation, directly at the exit of the accessory vein and below the bifurcation. These were then massaged with a finger massage for 10-15 seconds in the area of boththe varicose veins and also into the confluent accessory truncal vein. A compression bandage was then immediately applied here as well.
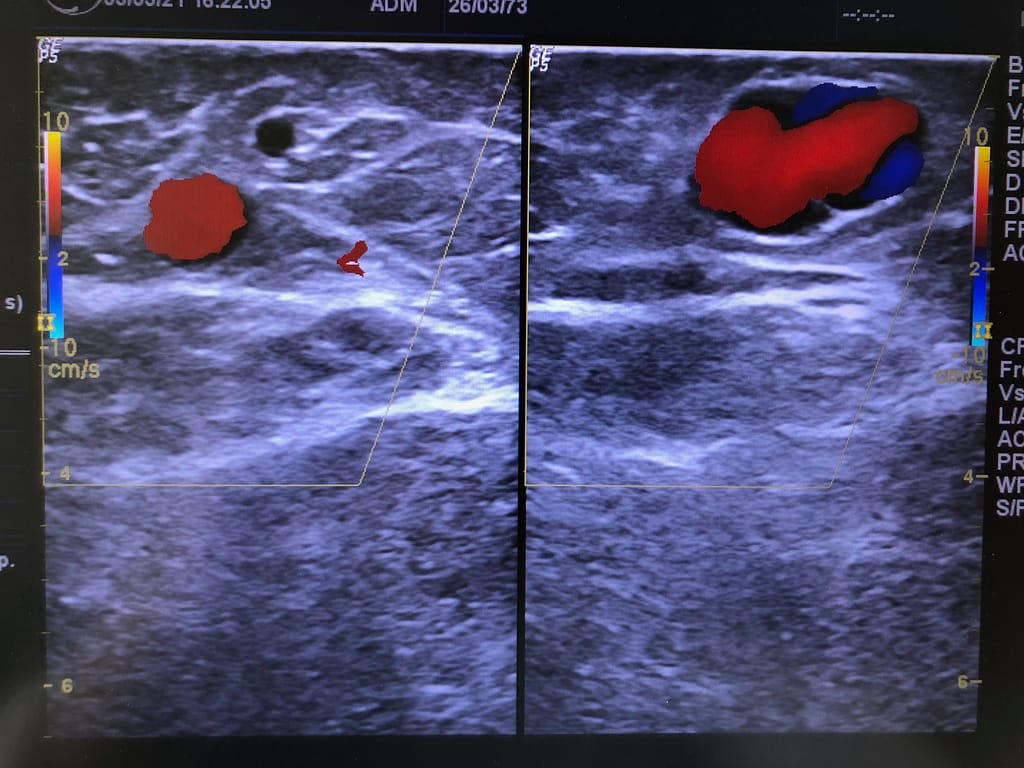
Die Duplex-Sonografie nach der Verklebung zeigt den effektiven Verschluss der Stammkrampfader und auch den Mündungsbereiches der akzessorischen Stammvene. Eine zusätzliche Injektion von Klebertropfen war hier nicht notwendig, die Fingermassage hatte zu einer vollständigen Benetzung der Gefäßgabel mit Kleber geführt (Bilder unten).
The duplex sonography after the sealing therapy shows the effective closure of the truncal varicose vein and also the opening area of the accessory truncal vein. An additional injection of drops of glue was not necessary here, as the finger massage resulted in the vascular fork being completely wetted with glue (pictures above).
Saphenion®: Venenkleber bei aneurysmatischen Krampfadern – Unser Resümeè
Anatomisch – pathologische Erweiterungen von Krampfadern sind nicht so selten, wie man vermuten kann. In unserem eigenen Patientenprotokoll finden sich seit 8 / 2012 bei 3105 mit Venenkleber operierten Stammkrampfadern 393 Stammvenen (12,7%) mit einer solchen beschriebenen Erweiterung. Der Durchmesser dieser Venen lag in jedem Fall über 1,5 cm. In all diesen Fällen wurde eine Therapie mit dem Venenkleber durchgeführt.
Bei den mittels klebendem Mikroschaum (Sealing Foam) behandelten ca. 1020 Stammvenen wurde als therapeutische Grenze ein Venendurchmesser von maximal 0,45 cm definiert. Stammvenenerweiterungen sind also keine Indikation für eine kathetergestützte Mikroschaumtherapie und finden sich deshalb in unserem Therapieprotokoll nicht.
Die Therapie einer aneurysmatischen Venenerweiterung stellt den Operateur bei jedem Therapieverfahren vor eine besondere Herausforderung. Blutungen, Gewebeverletzungen, Nervenläsionen, Lymphbahnverletzungen und Veneneinrisse sind hierbei nicht selten. Dies gilt insbesondere für die offene radikale Chirurgie des „Strippings“. Aber auch bei thermischen Verfahren ist eine höhere Energie -/ Wärmemenge notwendig um einen effektiven Verschluß der kranken Stammkrampfader zu erreichen. Auch dies birgt ein Risiko für Gewebeverletzungen in sich.
Somit ist der Venenkleber, bei entsprechenden Modifikationen des Therapieablaufs, eine sehr gute Behandlungsalternative auch bei aneurysmatisch veränderten Stammkrampfadern. Diese Erfahrung durften auch wir in den letzten fast 9 Jahren Einsatz mit dem VenaSeal®-Cloure – System machen. Eine Anpassung der Anzahl injizierten Klebertropfen (0,09 ml je Tropfen) und auch eine Modifikation der Distanz bei der Abgabe sind hier zu nennen. Zwingend ist weiterhin eine spezielle Lagerung des Patienten (Kopftieflagerung nach Trendelenburg) sowie die umgehende Anlage eines Kompressionsverbandes / Kompressionsstrumpfes. Unabhängig von diesen Modifikationen sind Narkose oder Tumeszenzanästhesie weiterhin nicht notwendig und eine sofortige Mobilisierung möglich.
Saphenion®: Vein glue for aneurysmal varicose veins – Summary
Anatomic-pathological enlargements of varicose veins are not as rare as one might suspect. In our own patient protocol, since 8/2012, there are 393 truncal varicose veins (12.7%) with such an enlargement described in 3105 varicose veins operated on with vein glue. The diameter of these veins was more than 1.5 cm in each case. In all of these cases, therapy with vein glue was carried out.
For the approx. 1020 saphenous veins treated with adhesive microfoam (sealing foam), a maximum venous diameter of 0.45 cm was defined as the therapeutic limit. Dilation of the trunk veins is therefore not an indication for catheter-supported microfoam therapy and is therefore not included in our therapy protocol.
The therapy of aneurysmal vein enlargement poses a special challenge for the surgeon with every therapy procedure. Bleeding, tissue injuries, nerve lesions, lymphatic tract injuries and vein tears are not uncommon. This is especially true for the radical open surgery of „stripping“. But even with thermal processes, a higher amount of energy/heat is necessary to achieve effective closure of the diseased truncal varicose vein. This also carries a risk of tissue damage.
Thus, the vein glue, with appropriate modifications of the therapy process, is a very good treatment alternative even for aneurysmally altered trunk varicose veins. We have been able to make this experience in the last almost 9 years of use with the VenaSeal®-Closure system. An adjustment of the number of injected drops of glue (0.09 ml per drop) and also a modification of the distance when dispensing should be mentioned here. Special positioning of the patient (head-down position according to Trendelenburg) as well as the immediate application of a compression bandage/compression stocking is imperative. Irrespective of these modifications, anaesthesia or tumescent/local anaesthesia is still not necessary and immediate mobilization is possible.

Photos: Utzius
Referenzen / Links:
Chan YC, Law Y, Cheung GC, Ting AC, Cheng SW. Cyanoacrylate glue used to treat great saphenous reflux: Measures of outcome. Phlebology. 2017 Mar;32(2):99-106. doi: 10.1177/0268355516638200. Epub 2016 Jul 9. PMID: 27052039.
Chan YC, Law Y, Cheung GC, Cheng SW. Predictors of Recanalization for Incompetent Great Saphenous Veins Treated with Cyanoacrylate Glue. J Vasc Interv Radiol. 2017 May;28(5):665-671. doi: 10.1016/j.jvir.2017.01.011. Epub 2017 Mar 8. PMID: 28284885.
Cho S, Gibson K, Lee SH, Kim SY, Joh JH. Incidence, classification, and risk factors of endovenous glue-induced thrombosis after cyanoacrylate closure of the incompetent saphenous vein. J Vasc Surg Venous Lymphat Disord. 2020 Nov;8(6):991-998. doi: 10.1016/j.jvsv.2020.01.009. Epub 2020 Mar 14. PMID: 32179036.
Gibson K, Ferris B. Cyanoacrylate closure of incompetent great, small and accessory saphenous veins without the use of post-procedure compression: Initial outcomes of a post-market evaluation of the VenaSeal System (the WAVES Study). Vascular. 2017 Apr;25(2):149-156. doi: 10.1177/1708538116651014. Epub 2016 Jul 9. PMID: 27206470.
Park I, Kim D. Correlation Between the Immediate Remnant Stump Length and Vein Diameter After Cyanoacrylate Closure Using the VenaSeal System During Treatment of an Incompetent Great Saphenous Vein. Vasc Endovascular Surg. 2020 Jan;54(1):47-50. doi: 10.1177/1538574419879563. Epub 2019 Oct 3. PMID: 31581906; PMCID: PMC6900567.
Park I. Successful use of VenaSeal system for the treatment of large great saphenous vein of 2.84-cm diameter. Ann Surg Treat Res. 2018 Apr;94(4):219-221. doi: 10.4174/astr.2018.94.4.219. Epub 2018 Mar 26. PMID: 29629358; PMCID: PMC5880981.
Kim J, Joh JH, Park HC. Effect of saphenous vein diameter and reflux time on stump length after cyanoacrylate closure. Exp Ther Med. 2019 Sep;18(3):1845-1849. doi: 10.3892/etm.2019.7758. Epub 2019 Jul 9. PMID: 31410146; PMCID: PMC6676198.
https://pubmed.ncbi.nlm.nih.gov/29629358/
https://pubmed.ncbi.nlm.nih.gov/32063522/
Ulf, can you please tell me the technique you used to deliver glue to venous aneurysm and maximum diameter of the aneurysm.
I have a very similar case pre treatment and was considering direct puncture with 16g IV and feed thin glue catheter thru this. Is this what you did ?
Did they get much inflammatory reaction after ?
Have you seen them again since ?
Yes I will do:
In the earlier time of sealing I did the same like You, direct punction with Seldinger needle into the aneurysm. but now I´m going inside the truncal vein only 1 cm and inject 2-3 drops of glue in the aneurysmatic part, digital pressure for 1 minute and then I´m going away ….