
Saphenion®: Venenkleber Unterschenkelkrampfadern 1. Wahl – 166 Monate Anwendung
Saphenion®: vein glue lower leg varicose 1st. choice – 166 months of use
Saphenion®: Venenkleber an Unterschenkelkrampfadern 1. Wahl – Bereits am 22.09.2014 veröffentlichten wir auf unserer Website unsere Einschätzung zum Einsatz des Venenklebers „VenaSeal®“ an den Stammkrampfadern des Unterschenkels (Vena saphena magna / Vena saphena parva, Vena femoropoplitea).
Damals in 2014 schrieben wir:
„Bei SAPHENION® wird seit dem 01.08.2012 mit dem Venaseal® – Closure – System gearbeitet. Bis zum 18.09.2014 wurden 572 Stammvenen behandelt, Es wurden 179 Parvavenen am Unterschenkel mit dem neuen Therapiesystem verklebt.
Unsere Erfahrungen zum Venaseal® – System durften wir auf der Jahrestagung der Deutschen Gesellschaft für Phlebologie im Rahmen eines Workshops vortragen. Hier haben wir o.g. Standpunkt zur Therapie der V. saphena parva (SSV) erstmals veröffentlicht. Hier unsere Zusammenfassung:
Bis zum 18.09.2014 wurden 179 Parvavenen ( SSV ) mit VenaSeal® verschlossen. Die Länge der behandelten Venen lag zwischen 18 – 30 cm. Für den Durchmesser der behandelten Venen wurden Werte zwischen 0,5 cm und 1 cm gemessen. In einem Fall wurde auch ein Mündungsaneurysma der v. saphena parva behandelt. Es wurden lediglich 25 Rekanalisationen der v. saphena parva duplexsonografisch nachgewiesen. Damit liegt die Effektivität der VenaSeal® – Verklebung von hinteren Stammkrampfadern ( V.saphena parva, SSV ) bei 98,9%.
Diese ausgezeichneten Ergebnisse werden nicht durch eine höhere Rate an Nebenwirkungen erkauft. Ganz im Gegenteil profitiert gerade die Behandlung der V. saphena parva von dem schonenden Venenkleben. Es fehlt – im Gegensatz zu Laser, Heissdampf oder der Radiowelle – jeder thermische oder elektrische Reiz auf Venenwand und Gewebe. Damit fallen die bei Laser, Heissdampf und Radiowelle gefürchteten neurologischen Nebenwirkungen nahezu komplett weg. Nur in 3 Fällen ( 1,7% ) fand sich post operativ eine leichte unspezifische Fremdkörperreaktion. Eine postoperative Pigmentation des subkutan gelegenen Venenstrangs wurde in keinem Fall beobachtet.
Auf Grund unserer Erfahrungen nach 26 Monaten Einsatz des VenaSeal®-Systems im Allgemeinen und an der V. saphena parva im Besonderen gilt für uns jetzt das VenaSeal® – Closure – Therapie als Methode der 1. Wahl bei der Behandlung der Parvavaricosis.„
Saphenion®: vein glue lower leg varicose 1st. choice – 166 months of use
Saphenion®: Vein glue on lower leg veins, first choice—On September 22nd, 2014, we published our assessment of the use of the vein glue „VenaSeal®“ on the truncal varicose veins, lower GSV and SSV / Fempop, on our website.
SAPHENION® has been working with the Venaseal® closure system since 08/01/2012. Until September 18, 2014, 572 truncal varicose veins had been treated. We treated 393 GSV and 179 SSV sealed with the therapy system vein glue.
We were able to present our experience of the Venaseal® system in a workshop at the annual conference of the German Society for Phlebology. Here we have the above position on the treatment of V. saphena parva (SSV) published for the first time. Here is our summary:
By September 18, 2014, 179 SSV had been closed with VenaSeal®. The length of the treated veins was between 18 – 30 cm. Diameters between 0.5 cm and 1 cm were seen for the vein diameter of treated varicose veins. In one case, an SSV aneurysm was treated. To date, only two recanalizations of the SSV were detected by duplex sonography. The effectiveness of VenaSeal® bonding of posterior varicose veins (SSV) is 98.9%.
A higher rate of side effects does not buy these excellent results. On the contrary, the treatment of the SSV benefits from the new gentle venous life. In contrast to lasers, hot steam, or radio waves, there is no thermal or electrical stimulus on the vein wall and tissue. This means that the neurological side effects feared by lasers, hot steam, and radio waves are almost eliminated. We found no patient with sensation or numbness in the lower leg. Only in 3 cases (1.7%) was there a mild non-specific inflammatory reaction of the tissue for 3-5 days postoperatively. Postoperative pigmentation of the subcutaneous cord was never observed.
Based on our experience after 26 months of using the VenaSeal® system in general and SSV in particular, we now consider VenaSeal® – Closure Therapy to be the first choice method in the treatment of lower led varicose veins GSV, SSV, and fempop varicose veins.
Saphenion: Vein glue on lower leg varicose veins – duplex 4 weeks after therapy
Saphenion®: Venenkleber Unterschenkelkrampfadern – 166 Monate Einsatz
Aktuell haben wir bis zum 09. 06. 2026 die Vena saphena parva in 1463 Fällen mit dem VenaSeal® – System therapiert und in 120 Fällen zusätzlich und simultan die Vena femoropoplitea (Verlängerung der Saphena parva zum Oberschenkel hin) mittels Venenkleber verschlossen.
Die Ergebnisse nach nunmehr 166 Monaten Einsatz rechtfertigen voll und ganz unsere damals aufgestellte These – der non tumescente, non thermale und non kompressive Venenkleber hat sich als Therapie der 1. Wahl für die Behandlung von Vena saphena parva und Vena femoropoplitea herausgestellt und unsere vor 12 Jahren veröffentlichte Meinung vollauf bestätigt!
Zusätzlich gilt nunmehr auch die Empfehlung für den Unterschenkelabschnitt der Vena saphena magna bei der Therapie von inkomplett entfernten Venen oder Rezidivkrampfadern der Vena saphena magna.
Wir sahen bisher bei 1463 behandelten Parvavenen eine Rekanalisation in 24 Fällen (1,7%). Somit beträgt die Behandlungseffektivität bei der hinteren Stammkrampfader am Unterschenkel 98,2%, dies über 13 Jahre betrachtet – und bleibt damit über den gesamten Untersuchungszeitraum nahezu unverändert.
Das Auftreten von Nebenwirkungen und Komplikationen hat sich im Verlauf der Therapie in keiner Weise verändert. Damit fallen die bei Laser, Heissdampf, Radiowelle und SONOVEIN (sofern diese Therapie überhaupt möglich ist) gefürchteten neurologischen Nebenwirkungen nahezu komplett weg.
Wir fanden keinen Patienten mit neurologisch bedingten Missempfindungen oder Taubheitsgefühl am Unterschenkel. Nur in 9 Fällen ( 0,7% ) fand sich post operativ eine leichte unspezifische Entzündungsreaktion des Gewebes für 3-5 Tage. Eine postoperative Pigmentation des subkutan gelegenen Venenstrangs sahen wir – wie zuvor bereits berichtet – weiterhin überhaupt nicht. In einem Fall sahen wir einen Kleberpickel.
Damit sehen wir uns in unseren frühen Erfahrungen nach Einsatz des Venenklebers „VenaSeal®“ nicht nur bestätigt – wir sehen diese Therapie jetzt – wie auch in den aktuellen europäischen und bundesdeutschen Leitlinien bestätigt – als „Gold-Standard“ bei der Parvavaricosis.
Saphenion®: Venenkleber Unterschenkelkrampfadern – Aktuelle Therapieleitlinien der Deutschen Gesellschaft für Venenheilkunde (DGP):
https://www.awmf.org/leitlinien/detail/ll/037-018.html
Auch die DGP sieht die Problematik thermischer Verfahren beim Einsatz an den Unterschenkelvenen (Nervenschädigung!) inzwischen ähnlich und hat in den aktuellen Leitlinien von 2019 /2020 auch in ihren Empfehlungen darauf reagiert.
Empfehlung 100: Um sensible Nervenschädigungen zu vermeiden kann es sinnvoll sein, die VSP nicht unterhalb der Wadenmitte thermisch zu behandeln.
Empfehlung 102: Die endovenös thermische Ablation soll unter dem Schutz eines perivenösen Flüssigkeitsmantels (Tumeszenzlösung) durchgeführt werden. Dieses Verfahren ist „off label use“ (keine Zulassung!).
Damit wird unsere Empfehlung von 2014 entsprechend bestätigt!


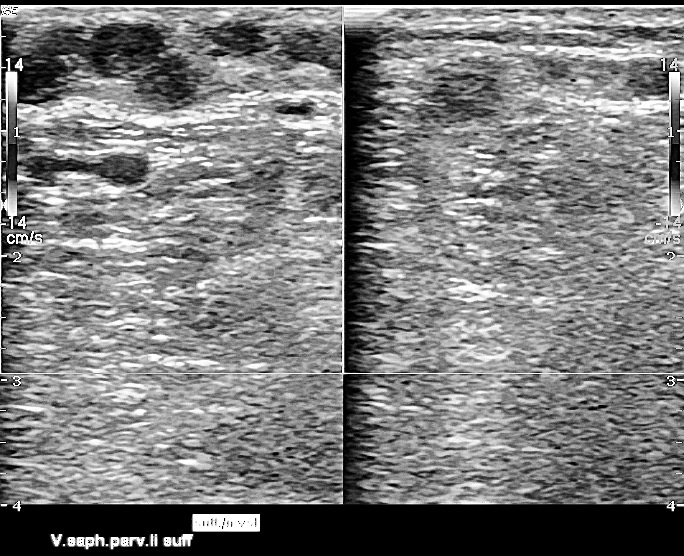
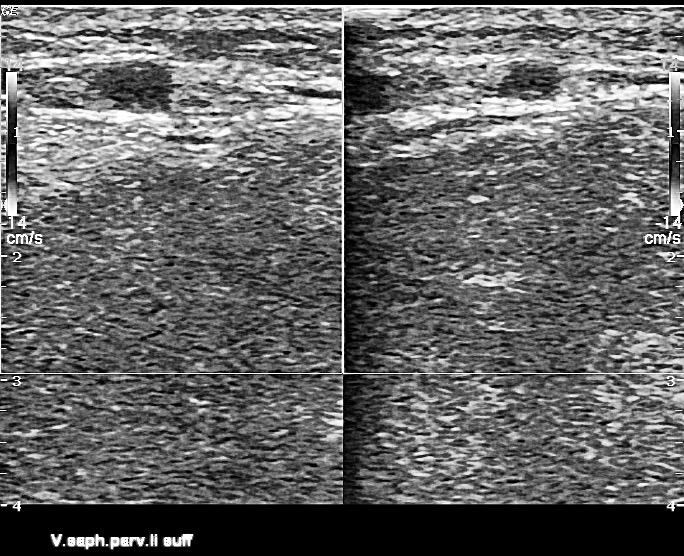
Saphenion®: Venenkleber an den Unterschenkelkrampfadern 1. Wahl – li. Bild: Kleben der VSM am Unterschenkel nach Stripping – Op inkomplett 20 Jahre zuvor, re. Bild: simultane Therapie an der VSP des gleichen Beines
Saphenion®: 1st choice vein glue on the varicose veins of the lower leg – left picture: Sealing the GSV on the lower leg after stripping – incomplete operation 20 years earlier, right picture: simultaneous therapy on the SSV of the same leg.
Saphenion®: Vein glue lower leg varicose veins SSV / Fempop – 166 months in use
Up to June, 09. 06. 2026, we treated the SSV in 1463 cases and 120 cases additionally and simultaneously closed the femoropopliteal vein (extension of the saphenous parva to the thigh) with vein glue.
The results after 166 months usefully justified our thesis at the time – the non-tumescent, non-compressive, and non-compressive vein glue has emerged as the first-choice therapy for the treatment of the lower leg saphenous vein and femoropopliteal vein and fully confirmed our opinion published 12 years ago!
In addition, the recommendation now also applies to the lower leg section of the greater saphenous veins in the treatment of incompletely removed veins or recurrent varicose veins of the GSV.
We have treated 1463 SSV and seen recanalizations in 24 cases. The treatment effectiveness of the posterior varicose vein on the lower leg is 98.2%, viewed over 166 months, and thus remains almost unchanged over the entire investigation period.
The occurrence of side effects and complications has not changed during therapy. This means that the neurological side effects feared by lasers, hot steam, radio waves, and SONOVEIN (if this therapy is possible at all) are almost eliminated.
We did not find any patients with neurological disorders or numbness in the lower leg. Only in 9 cases (0,7%) was there a mild non-specific inflammatory reaction of the tissue for 3-5 days postoperatively. As previously reported, we did not see any postoperative pigmentation of the subcutaneous tissue. In one case we saw a glue pick.
In our early experiences after using the vein glue „VenaSeal®“ we not only see this confirmed – we think this therapy is the „gold standard“ for SSV and Femoropopliteal veins.
Saphenion®: Venous glue lower leg varicose veins – Current therapy guidelines of the German Society for Venous Medicine (DGP):
https://www.awmf.org/leitlinien/detail/ll/037-018.html
The DGP now also sees the problem of thermal procedures when used on the lower leg veins (nerve damage!) And has reacted to this in the current guidelines of 2019 in its recommendations.
Recommendation 100: To avoid sensitive nerve damage, it can make sense not to treat the VSP below the middle of the calf thermally.
Recommendation 102: Endovenous thermal ablation should be carried out under the protection of a perivenous liquid jacket (tumescent solution). This procedure is „off-label use“ (no approval!).
This confirms our recommendation from 2014 accordingly.
Saphenion® Rostock: Toni Krahl in der Kunsthalle Rostock
Photos /Video: Saphenion, Utzius
Papers / Links:
Almeida JI, Murray SP, Romero ME. Saphenous vein histopathology 5.5 years after cyanoacrylate closure. J Vasc Surg Venous Lymphat Disord. 2020 Mar;8(2):280-284. doi: 10.1016/j.jvsv.2019.04.014. Epub 2019 Jul 4. PubMed PMID: 31281102.
Kolluri R, Chung J, Kim S, Nath N, Bhalla BB, Jain T, Zygmunt J, Davies A. Network meta-analysis to compare VenaSeal with other superficial venous therapies for chronic venous insufficiency. J Vasc Surg Venous Lymphat Disord. 2020 Feb 13. pii: S2213-333X(19)30702-4. doi: 10.1016/j.jvsv.2019.12.061. [Epub ahead of print] Review. PubMed PMID: 32063522.
Gibson K, Minjarez R, Gunderson K, Ferris B. Need for adjunctive procedures following cyanoacrylate closure of incompetent great, small and accessory saphenous veins without the use of postprocedure compression: Three-month data from a postmarket evaluation of the VenaSeal System (the WAVES Study). Phlebology. 2019 May;34(4):231-237. doi: 10.1177/0268355518801641. Epub 2018 Sep 18. PubMed PMID: 30227791.
Gibson K, Morrison N, Kolluri R, Vasquez M, Weiss R, Cher D, Madsen M, Jones A. Twenty-four month results from a randomized trial of cyanoacrylate closure versus radiofrequency ablation for the treatment of incompetent great saphenous veins. J Vasc Surg Venous Lymphat Disord. 2018 Sep;6(5):606-613. doi: 10.1016/j.jvsv.2018.04.009. Epub 2018 Jun 15. PubMed PMID: 29914814.
Park I. Initial Outcomes of Cyanoacrylate Closure, VenaSeal System, for the Treatment of the Incompetent Great and Small Saphenous Veins. Vasc Endovascular Surg. 2017 Nov;51(8):545-549. doi: 10.1177/1538574417729272. Epub 2017 Oct 2. PubMed PMID: 28969499.
Lam YL, De Maeseneer M, Lawson J, De Borst GJ, Boersma D. Expert review on the VenaSeal® system for endovenous cyano-acrylate adhesive ablation of incompetent saphenous trunks in patients with varicose veins. Expert Rev Med Devices. 2017 Oct;14(10):755-762. doi: 10.1080/17434440.2017.1378093. Review. PubMed PMID: 28892412.
Morrison N, Gibson K, Vasquez M, Weiss R, Jones A. Five-year extension study of patients from a randomized clinical trial (VeClose) comparing cyanoacrylate closure versus radiofrequency ablation for the treatment of incompetent great saphenous veins. J Vasc Surg Venous Lymphat Disord. 2020 Mar 20. pii: S2213-333X(20)30105-0. doi: 10.1016/j.jvsv.2019.12.080. [Epub ahead of print] PubMed PMID: 32205125.
Proebstle TM, Alm J, Rasmussen L, Dimitri S, LawsonJA, WhiteleyM,, Franklin IJ, Davies AH: The European Multicenter Study On Cyanoacrylate Embolization Of Refluxing Great Saphenous Veins Without Tumescent Anaesthesia And Compression Therapy. eScope – study; Abstract presented to the American Venous Forum Annual Meeting 2013, Phoenix ( AZ) the USA
Thum, J: Single Center Erfahrungen aus 234 Stammvenenbehandlungen mit viskösem n – Butyl – 2 – Cyanoacrylat- Verwendbarkeit, Akzeptanz, Ergebnisse; vasomed 1, 2019; 28 – 31
Üdris, Ints: 6 years single center results „Baltic Vein Clinic“ of truncal varicose vein sealing; Presentation on 2nd. NEEF, Riga, 17th. August 2019.
Zierau U Th.: Venenverklebung versus Radiofrequenztherapie bei Varicosis – Verlaufsstudie über 36 Monate mit 1139 Behandlungen. vasomed 28 (2016) 212 – 216.
Zierau UT and Lahl W: Recurrence Discussion in Varicose Veins Therapy – A Critical Examination of the Vein Stump discussion; J. Vasc. Endovasc. Therapy 2019, Vol.4 No.2:13
https://www.awmf.org/leitlinien/detail/ll/037-018.html
https://www.saphenion.de/news/saphenion-165-monate-langzeittherapie-venenkleber