
Saphenion® – Therapie von Perforanzkrampfadern mit Venenkleber: Klinische Bedeutung
Saphenion® – therapy of perforator varicose veins with vein glue: clinical significance


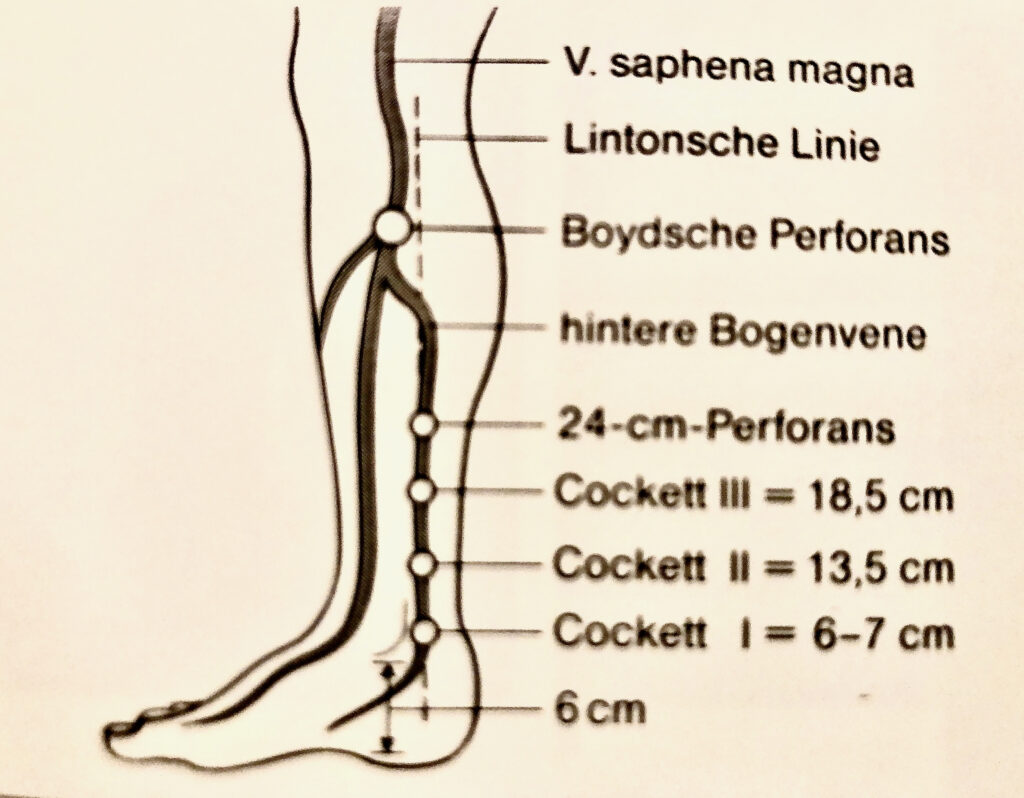
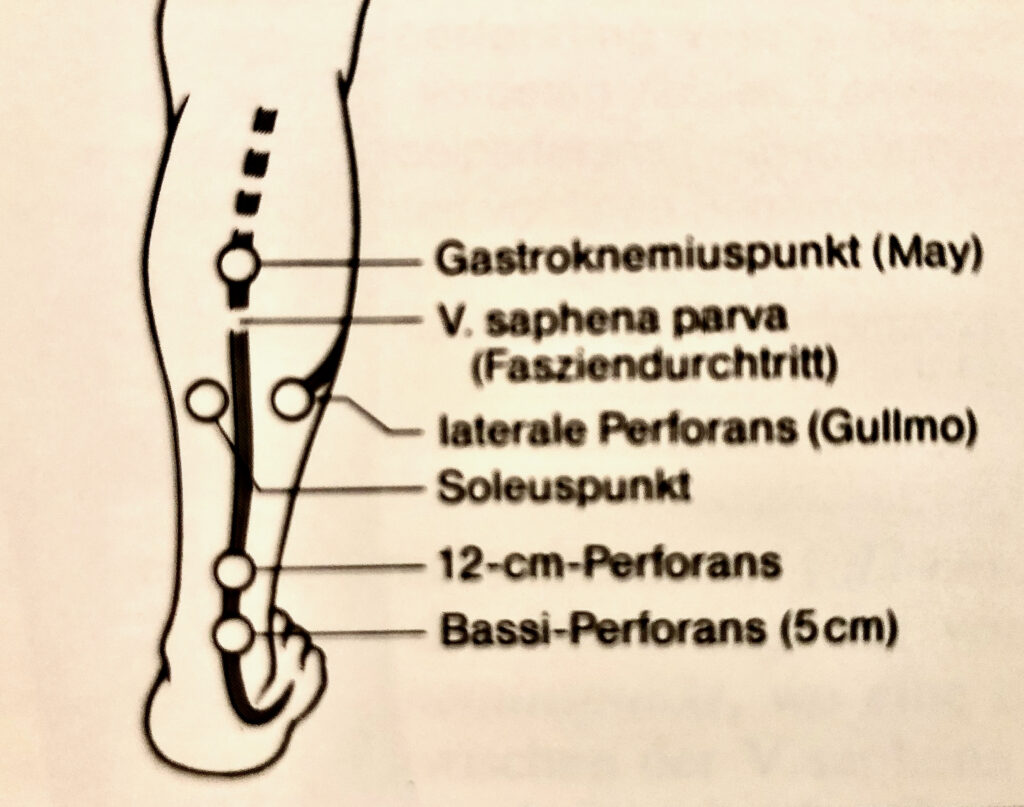
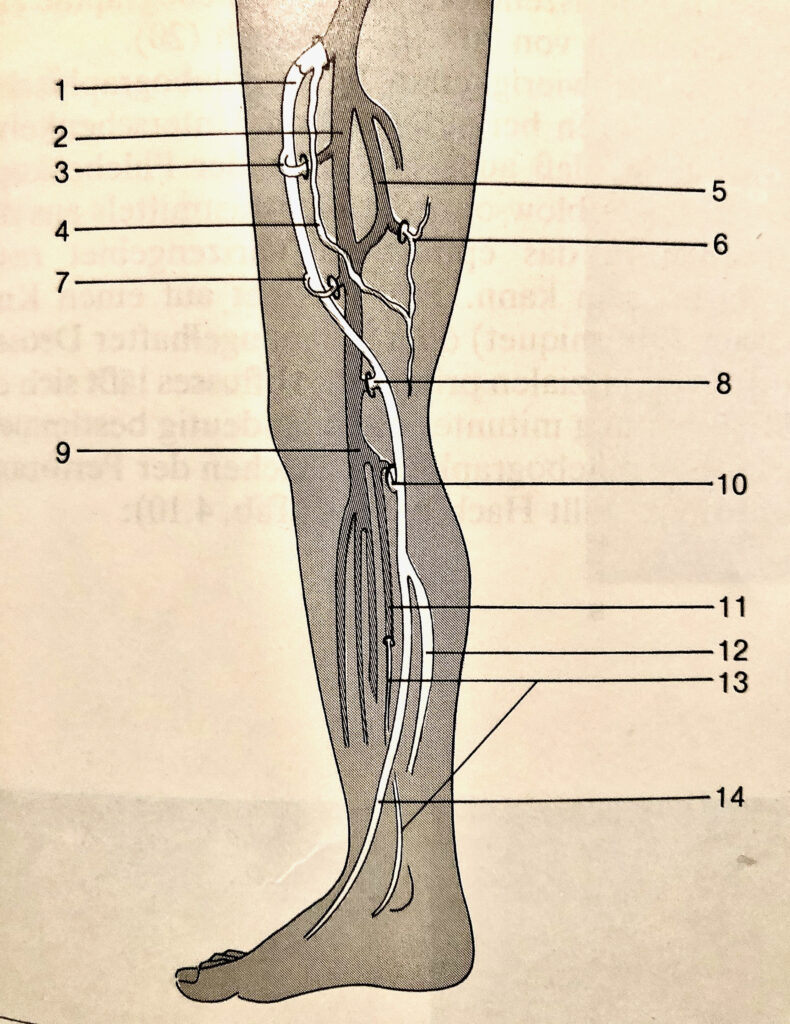
Saphenion® – Therapie von Perforanzkrampfadern mit Venenkleber: Das menschliche Venensystem hat etwa 140 Perforanz – Venenpaare, davon liegt die Mehrzahl am Unterschenkel. Von diesen Verbindungsvenen haben etwa 18-20 Venenpaare eine klinische Bedeutung. Deshalb werden sie auch Schlüsselperforanzvenen genannt. In über 60% der Fälle treten diese Venen als Paar auf und begleiten Hautarterien beim Durchtritt durch Muskelfaszien zur Haut.
Die Verbindungsvenen haben in der Regel Venenklappen, die den Blutstrom in Richtung des tiefen Venensystems lenken. Eine Ausnahme bilden die Verbindungsvenen am Fußrücken und im Knöchelbereich. Diese sind anatomisch und physiologisch ohne Venenklappen angelegt, haben also keine Funktion als Blutstromrichter. Hier pendelt das Blut somit je nach Stellung des Beines und Haltung des Fusses in Knöchel – und Fußsohlenrichtung hin und erzeugt einen erheblich erhöhten Venendruck am Sprunggelenk und Fußrücken / Fußsohle .
Die besondere Bedeutung der Verbindungsvenen liegt zum Einen in der Verbindung von tiefen Stammvenensystem zum Hautstammvenensystem (V.saphena magna und V. saphena parva, Vena akzessoria und Vena femoropoplitea), zum Anderen in der Drainage aus den Muskel – und Faszienvenen in den Hautvenenstamm.
Im Falle defekter Venenklappen in den Verbindungsvenen (Perforanzvenen) können lokale oder generalisierte Hautvenenkrampfadern am gesamten Bein entstehen. Die defekten Perforanzvenen potenzieren dabei den Grad bereits vorhandener hämodynamischer Störungen der Stammkrampfadern und führen zu deutlich verstärkten pathologischen (funktionellen und anatomischen) Effekten am Bein, insbesondere am Unterschenkel. Dies sind vor allem Haut – und Unterhautverhärtungen, Braun/Rotverfärbungen und schließlich das “Offene Bein” (Ulcus cruris).
Saphenion® – therapy of perforator varicose veins with vein glue: The human venous system has around 140 pairs of perforating veins, the majority of which are located on the lower leg. Of these connecting veins, about 18-20 pairs of veins are of clinical importance. That is why they are also called key perforation veins. In more than 60% of cases, these veins appear as a pair and accompany the skin arteries as they pass through muscle fascia to the skin.
The connecting veins usually have valves that direct blood flow toward the deep venous system. The connecting veins on the back of the foot and in the ankle area are an exception. These are anatomically and physiologically designed without vein valves, so they have no function as blood flow regulators. Here, depending on the position of the leg and the posture of the foot, the blood shuttles in the direction of the ankle and sole of the foot and generates a considerably increased venous pressure.
The particular importance of the perforator veins lies on the one hand in the connection of the deep truncal vein system to the cutaneous truncal vein system (V. saphena Magna, GSV – and V. saphena Parva, SSV – vena accessory and vena femoropopliteal) and on another hand in the drainage from the muscle and fascia veins into the cutaneous truncal veins. In the case of defective vein valves in the connecting veins (perforator veins), local or generalized cutaneous varicose veins can develop on the entire leg.
The defective perforator veins increase the degree of hemodynamic disorders of the truncal varicose veins that are already present and lead to significantly increased pathological (functional and anatomical) effects on the leg, especially on the lower leg. These are primarily hardened skin and subcutaneous tissue, brown/red discoloration and finally the “open leg” (ulcus cruris).
Saphenion® – Therapie von Perforanzkrampfadern mit Venenkleber: Die Therapieoptionen
Saphenion® – therapy of perforator varicose veins with venous glue: the therapy options
Die Therapie von Perforansvenen (Verbindungsvenen) wird in aller Regel entweder radikalchirurgisch / endoskopisch über diverse Hautschnitte durchgeführt oder aber es kommen Kathetersysteme (Laser / Radiowelle) zum Einsatz. In den letzten 10 Jahren ist auch die Mikroschaumtherapie für die Therapie der Verbindungsvenen wichtig geworden.
Bei den radikalchirurgischen Methoden ist neben der chirurgischen Radikalität immer eine Lokal – / Tumeszensanästhesie notwendig. Gleiches gilt für die endovenösen Verfahren Laser und Radiowelle. Einzig der Mikroschaum kommt ohne eine Schmerz – / Narkosetherapie aus.
Es gibt aber auch sehr kräftige Verbindungsvenen (Durchmesser > 5 mm), die entweder einen grossen radikalen Eingriff erforderlich machen, oder aber mittels der gängigen Kathetersysteme und mittels Mikroschaum nicht mehr effektiv verschlossen werden können. Auch das Risiko von postoperativen Thrombosen im tiefen Venensystem ist hier nicht zu verleugnen.
Wir hatten bereits 2018 von der Möglichkeit berichtet, mittels des VenaSeal® – Venenklebers auch lokale Befunde, so u.a. die für die Entstehung und den pathologischen Fortgang der Krampfadern wichtigen Perforanzvenen behandeln zu können.
The therapy of perforator veins (connecting veins) is usually carried out either by radical surgery / endoscopically via various skin incisions or catheter systems (laser/radio wave) are used. In the last 10 years, microfoam therapy has also become important for the therapy of connecting veins.
With radical surgical methods, local/tumescent anesthesia is always necessary in addition to surgical radicalism. The same applies to the endovenous laser and radio wave procedures. Only the microfoam does not require pain/anesthesia therapy.
But there are also very strong connecting veins (diameter > 5mm), which either require a major radical intervention or can no longer be effectively closed using conventional catheter systems and microfoam. Here, too, the risk of postoperative thrombosis in the deep venous system cannot be denied.
As early as 2018, we reported on the possibility of using the VenaSeal® – vein glue to treat local findings, including the perforating veins that are important for the development and pathological progression of varicose veins.
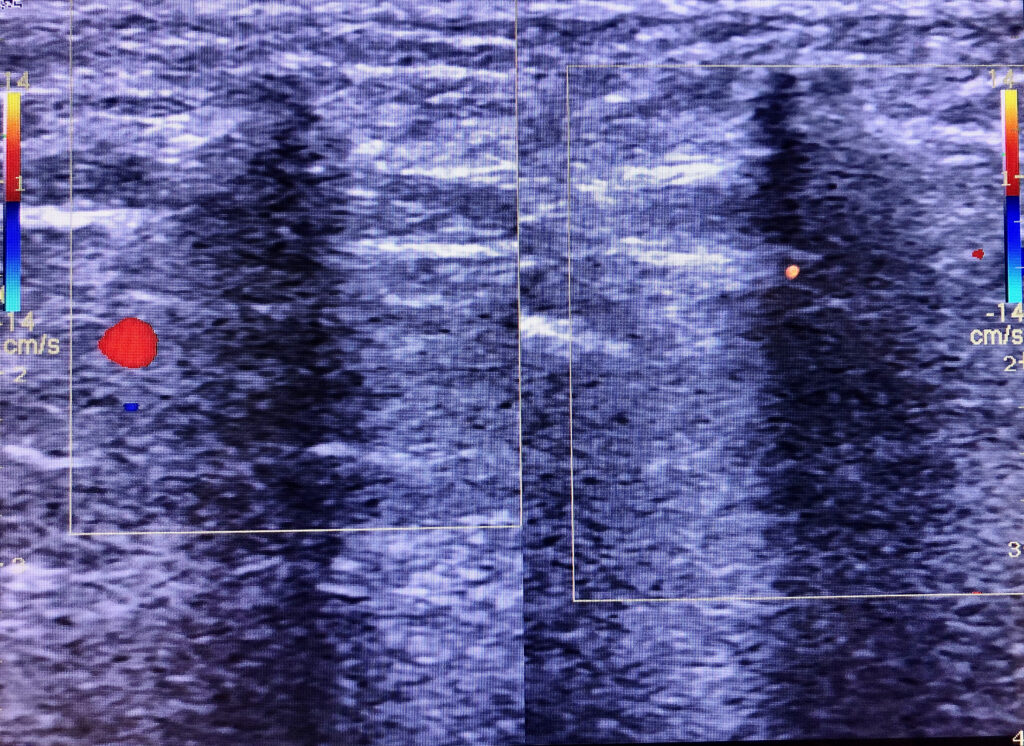
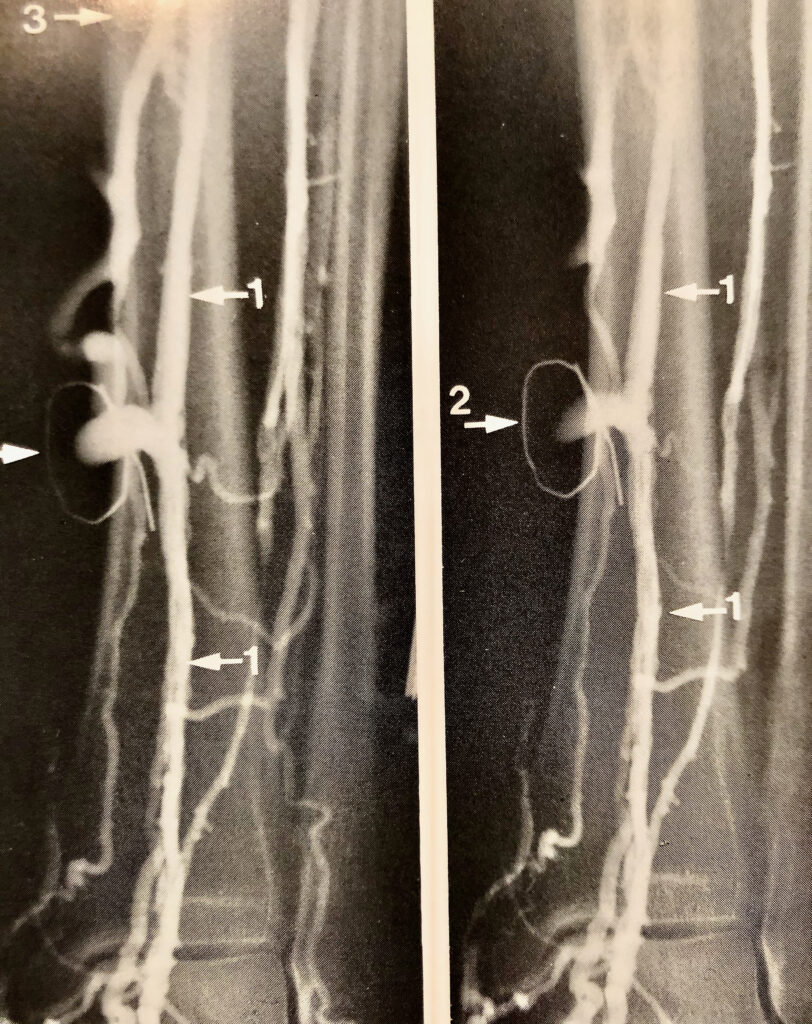
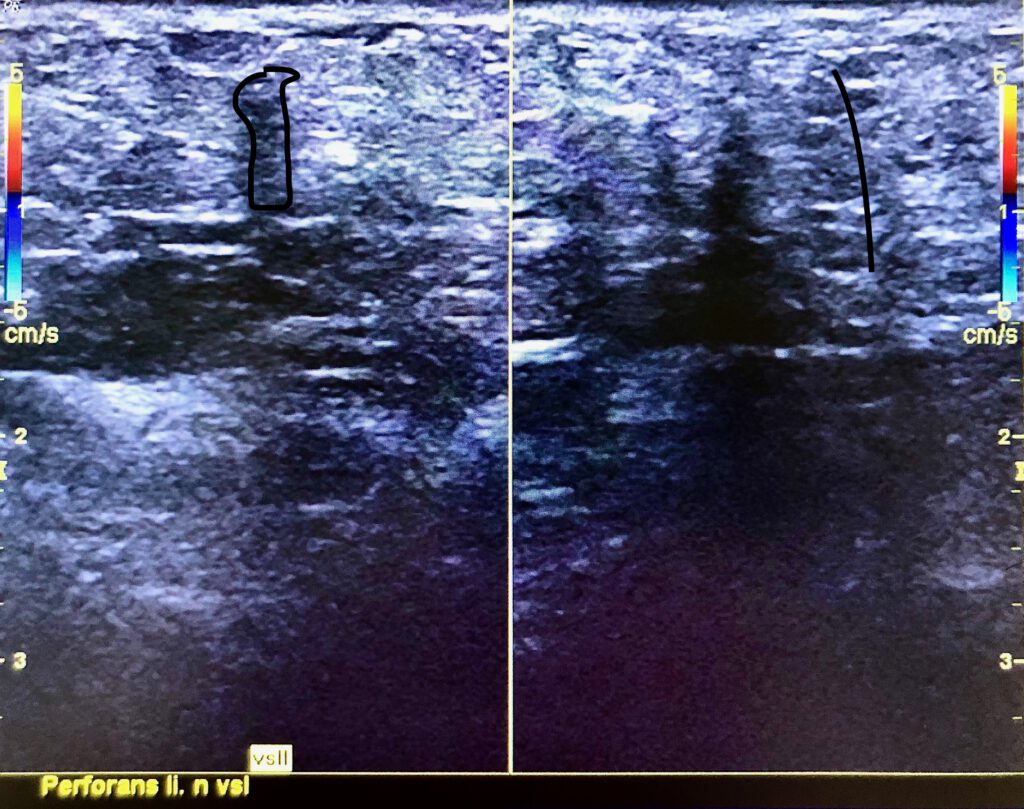
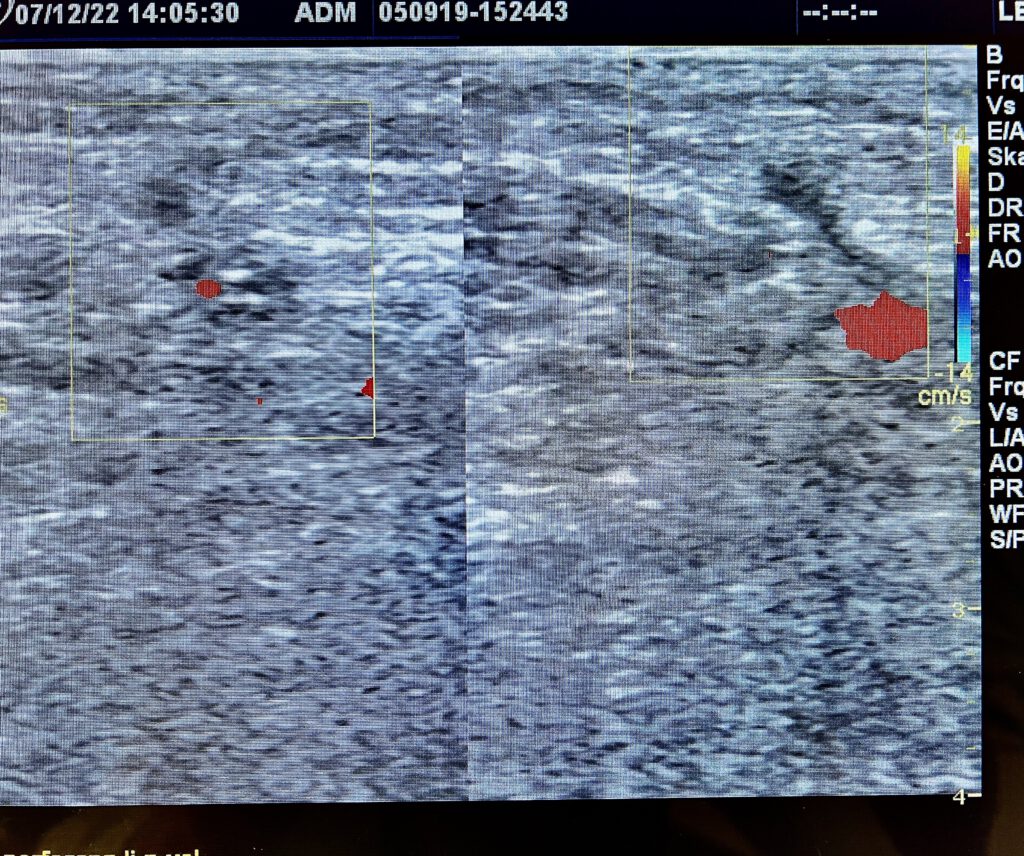
Saphenion® – therapy of perforator varicose veins with vein glue: Cockett 3 perforator vein before and after glue therapy. Sealed Bassi – perforator vein
Saphenion® – Therapie von Perforanzkrampfadern mit Venenkleber: Unsere Erfahrung
Saphenion® – therapy of perforating varicose veins with vein glue: Our Experience
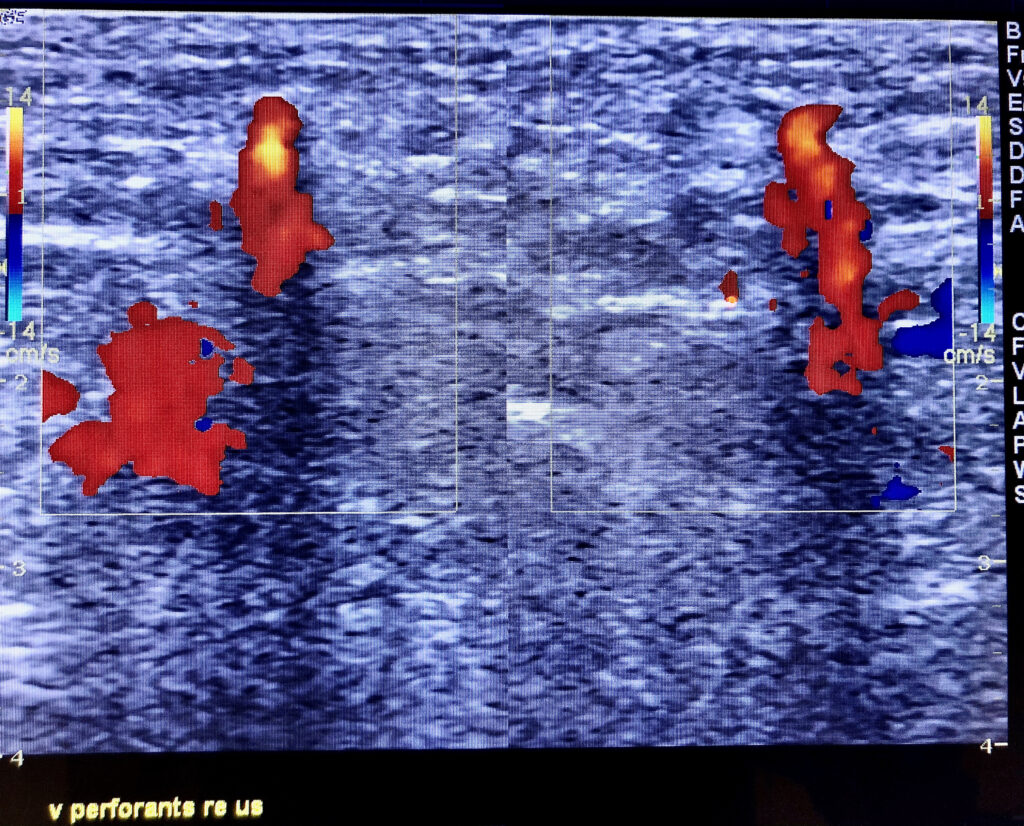
Saphenion® – Therapie von Perforanzkrampfadern mit Venenkleber: Diese Technik ergibt eine elegante und sichere Möglichkeit, die Perforanzvenen zeitgleich, zusammen mit der Therapie der Stammkrampfadern, mittels Venenkleber zu verschliessen. Zum Einen werden Perforanzvenen bereits beim Kathetermanöver in der Stammvene durch Abgabe eines zusätzlichen Klebertropfens an der Mündung (Ultraschallkontrolle!) verschlossen. Zum Anderen wird von uns nach Verklebung der Stammvenen in gleicher Sitzung mit der auf dem Op – Tisch liegenden Punktionsnadel auch die Perforanzvene direkt unter Sicht punktiert und verklebt.
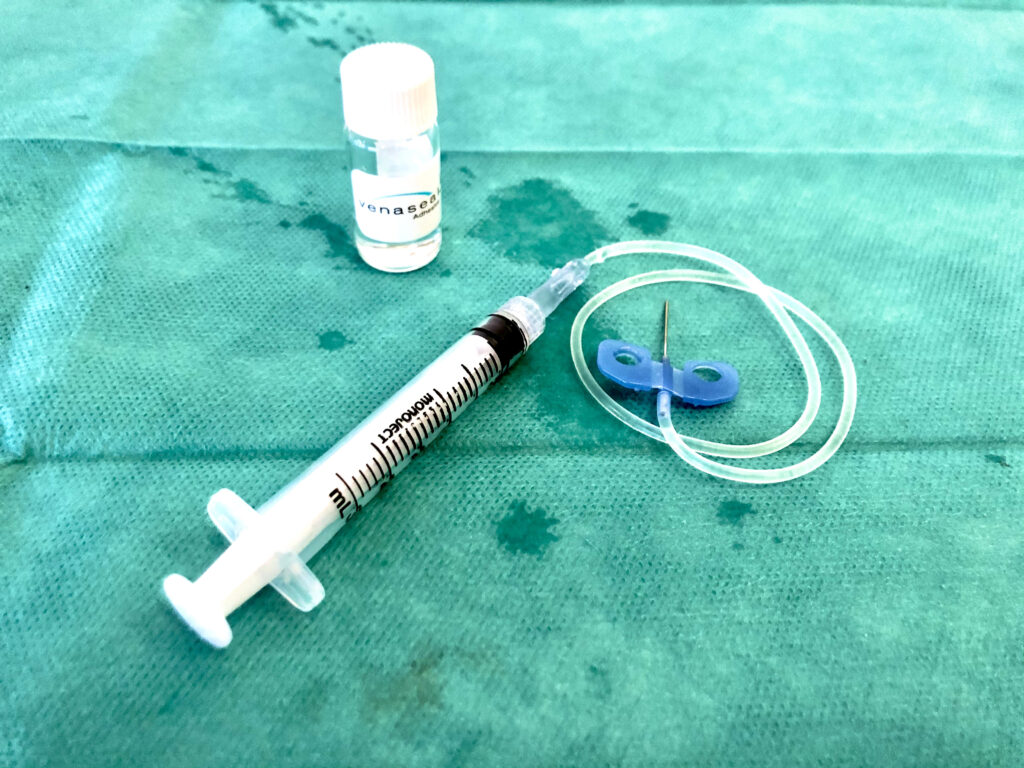
Unter duplexsonografischer Sicht werden 1 – 3 Klebertropfen (0,09-0,27ml) unter sonografischer Sichtkontrolle injiziert und nach dem notwendigen 60 Sekunden Druck auf die Perforanzvene ist diese Vene effektiv verschlossen. Der Vorteil hierbei ist die fehlende thermische Belastung. Damit besteht auch kein Risiko mehr für Nerven – und Lymphbahnschäden. Des Weiteren ist eine Lokal – oder Tumeszenzflächenanästhesie ebenfalls nicht notwendig.
Die Gefahr eines Eintropfens von Kleber in eine tiefe Vene oder Muskelvene ist bei exakter sonografischer Kontrolle und ausreichend Erfahrung beim Arbeiten mit dem Venenkleber verschwindend gering. Die gilt allerdings nur für den dickflüssigen VenaSeal® – Kleber, wässrige Kleber dürften bei dieser Indikation problematisch sein.
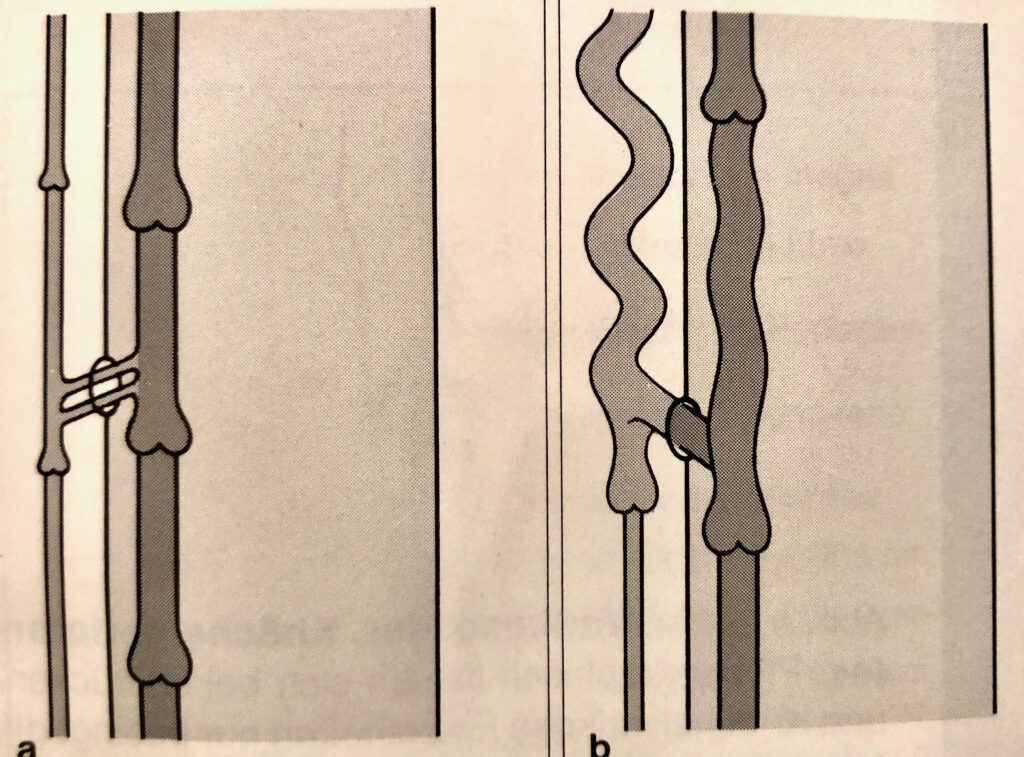
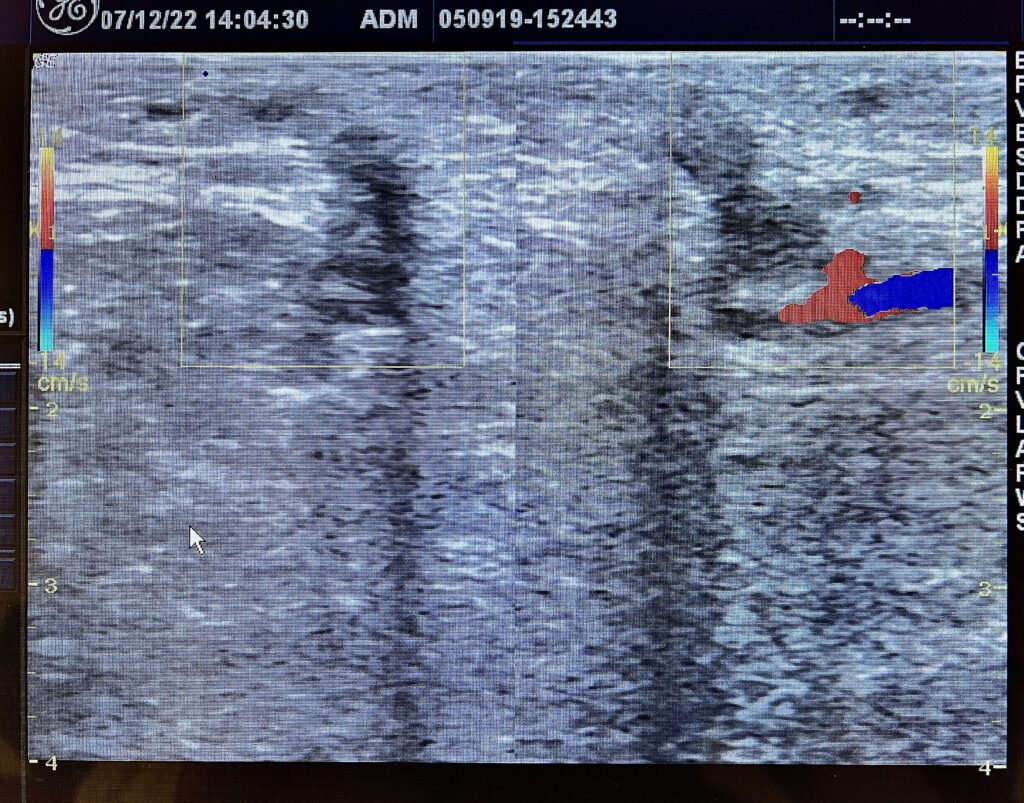
Sealing a perforator vein after treatment of both GSV with vein glue
Saphenion® – therapy of perforator varicose veins with vein glue: This technique provides an elegant and safe way to close the perforating veins at the same time as the therapy of the truncal varicose vein with vein glue. On the one hand, perforation veins are closed in the truncal veins during the catheter maneuver by dispensing an additional drop of glue at the mouth (ultrasound control!). On the other hand, after sealing the truncal saphenous veins, in the same session with the puncture needle lying on the operating table, we also puncture and glue the perforator vein directly under the sight.
Under the duplex sonographic vision, 1 – 3 drops of glue (0.09-0.27 ml) are injected under sonographic visual control and after the necessary 60 seconds of pressure on the perforant vein, the vein is effectively closed. The advantage here is the lack of thermal stress. This means that there is no longer any risk of nerve and lymphatic damage. Furthermore, local or tumescent surface anesthesia is also not necessary.
The risk of glue dripping into a deep vein or muscle vein is negligible with exact sonographic control and sufficient experience in working with the vein glue. However, this only applies to the viscous VenaSeal® adhesive, water-based glues are likely to be problematic for this indication.

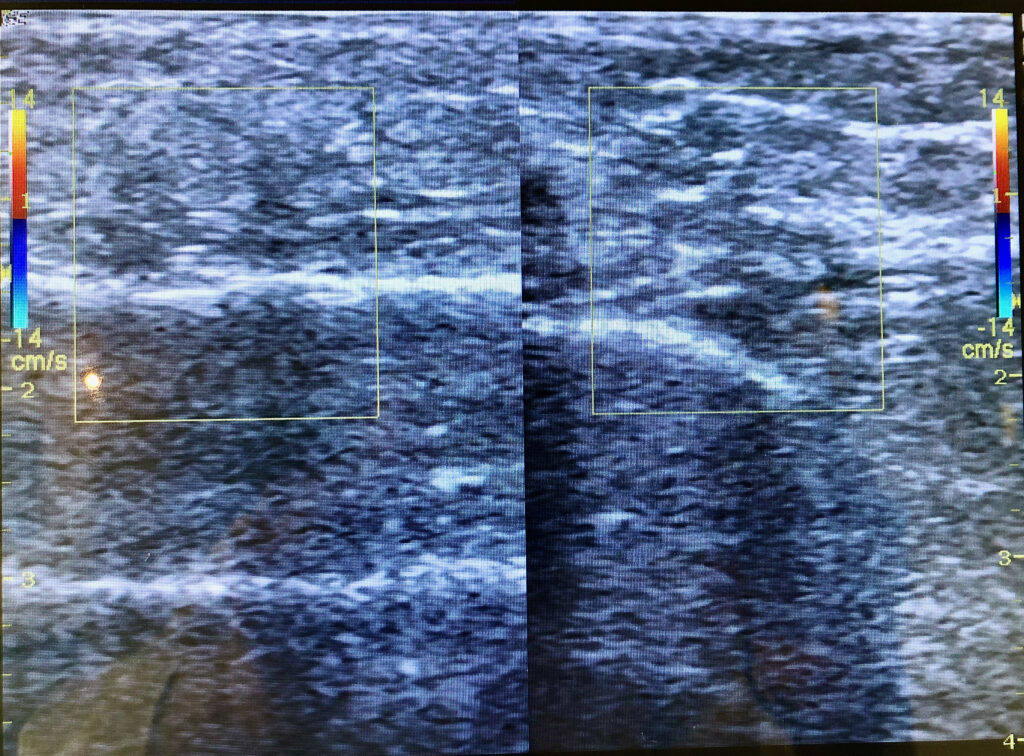

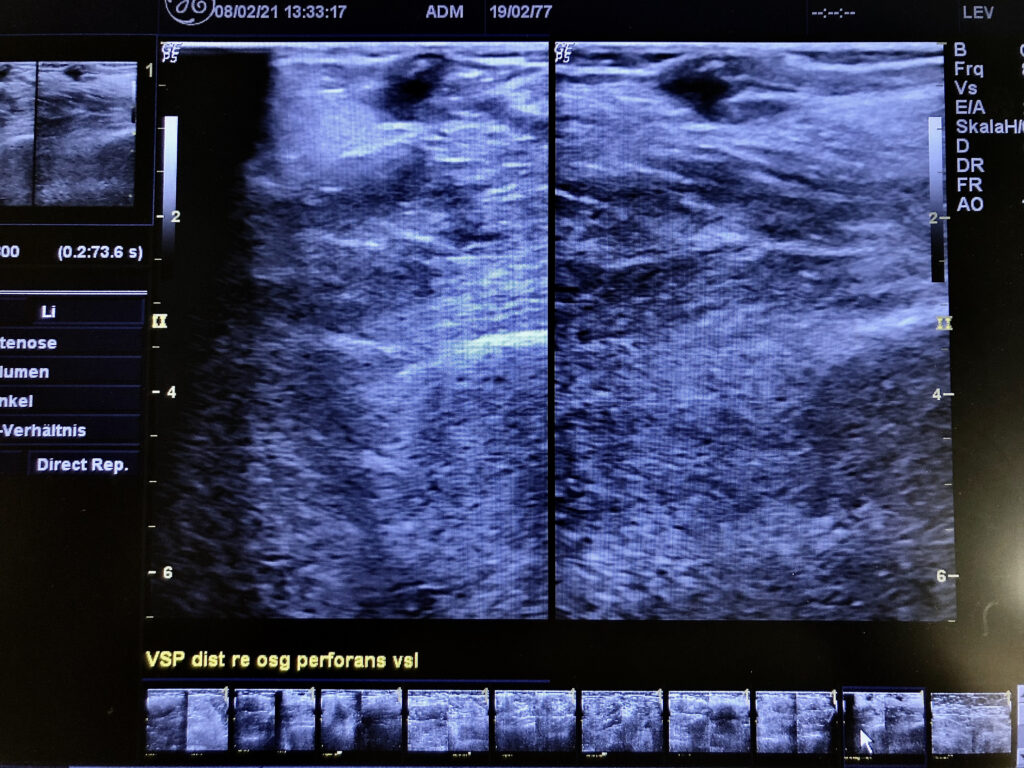
Saphenion® – Therapie von Perforanzkrampfadern mit Venenkleber: Befund nach 4 Wochen – Klinisch und im Ultraschall Verbindungsvenen verschlossen, Patient sehr zufrieden!
Saphenion® – Therapy of perforator varicose veins with vein glue: Findings after 4 weeks – Clinically and on ultrasound perforator veins closed, patient very satisfied!

Fotos /Videos: Claudia, Utzius
Papers / Links:
Aurshina A, Alsheekh A, Kibrik P, Hingorani A, Marks N, Ascher E. Recanalization After Endovenous Thermal Ablation. Ann Vasc Surg. 2018 Oct;52:158-162. doi: 10.1016/j.avsg.2018.03.017. Epub 2018 May 17. PMID: 29777845.
Bellam Premnath KP, Joy B, Raghavendra VA, Toms A, Sleeba T. Cyanoacrylate adhesive embolization and sclerotherapy for primary varicose veins. Phlebology. 2018 Sep;33(8):547-557. doi: 10.1177/0268355517733339. Epub 2017 Sep 28. PMID: 28956692.
Boersma D, Smulders DL, Bakker OJ, van den Haak RF, Verhoeven BA, Koning OH. Endovenous laser ablation of insufficient perforating veins: Energy is key to success. Vascular. 2016 Apr;24(2):144-9. doi: 10.1177/1708538115587214. Epub 2015 May 12. PMID: 25972028.
Burleva EP, Tiurin SA, Smirnov OA, Faskhiev RR. Sravnitel’nye trekhletnie rezul’taty flebéktomiĭ i termoablatsiĭ pri varikoznoĭ bolezni nizhnikh konechnosteĭ [Comparative 3-year results of phlebectomy and thermal ablation for lower limb varicose veins]. Angiol Sosud Khir. 2018;24(2):82-91. Russian. PMID: 29924778.
Chait J, Kibrik P, Alsheekh A, Ostrozhynskyy Y, Marks N, Rajaee S, Hingorani A, Ascher E. Radiofrequency Ablation Increases the Incidence of Endothermal Heat-Induced Thrombosis. Ann Vasc Surg. 2020 Jan;62:263-267. doi: 10.1016/j.avsg.2019.05.059. Epub 2019 Aug 5. PMID: 31394220.
Deak ST. Retrograde administration of ultrasound-guided endovenous microfoam chemical ablation for the treatment of superficial venous insufficiency. J Vasc Surg Venous Lymphat Disord. 2018 Jul;6(4):477-484. doi: 10.1016/j.jvsv.2018.03.015. PMID: 29909854.
Gibson K, Elias S, Adelman M, Hager ES, Dexter DJ, Vayuvegula S, Chopra P, Kabnick LS. A prospective safety and effectiveness study using endovenous laser ablation with a 400-μm optical fiber for the treatment of pathologic perforator veins in patients with the advanced venous disease (SeCure trial). J Vasc Surg Venous Lymphat Disord. 2020 Sep;8(5):805-813. doi: 10.1016/j.jvsv.2020.01.014. Epub 2020 Mar 21. PMID: 32205128.
Yang GK, Parapini M, Gagnon J, Chen JC. Comparison of cyanoacrylate embolization and radiofrequency ablation for the treatment of varicose veins. Phlebology. 2019 May;34(4):278-283. doi: 10.1177/0268355518794105. Epub 2018 Aug 16. PMID: 30114987.
Yao P, Mukhdomi T. Varicose Vein Endovenous Laser Therapy. 2020 Nov 30. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan–. PMID: 32491651.
Kolluri R, Chung J, Kim S, Nath N, Bhalla BB, Jain T, Zygmunt J, Davies A. Network meta-analysis to compare VenaSeal with other superficial venous therapies for chronic venous insufficiency. J Vasc Surg Venous Lymphat Disord. 2020 May;8(3):472-481.e3. doi: 10.1016/j.jvsv.2019.12.061. Epub 2020 Feb 14. PMID: 32063522.
Lawrence PF, Hager ES, Harlander-Locke MP, Pace N, Jayaraj A, Yohann A, Kalbaugh C, Marston W, Kabnick L, Saqib N, Pouliot S, Piccolo C, Kiguchi M, Peralta S, Motaganahalli R. Treatment of superficial and perforator reflux and deep venous stenosis improves healing of chronic venous leg ulcers. J Vasc Surg Venous Lymphat Disord. 2020 Jul;8(4):601-609. doi: 10.1016/j.jvsv.2019.09.016. Epub 2020 Feb 21. PMID: 32089497.
Proebstle T, van den Bos R. Endovenous ablation of refluxing saphenous and perforating veins. Vasa. 2017 May;46(3):159-166. doi: 10.1024/0301-1526/a000610. Epub 2017 Feb 27. PMID: 28238282.
Reitz KM, Salem K, Mohapatra A, Liang NL, Avgerinos ED, Singh MJ, Hager E. Complete Venous Ulceration Healing after Perforator Ablation Does Not Depend on Treatment Modality. Ann Vasc Surg. 2021 Jan;70:109-115. doi: 10.1016/j.avsg.2020.06.051. Epub 2020 Jun 27. PMID: 32603845; PMCID: PMC7744434.
Seren M, Dumantepe M, Fazliogullari O, Kucukaksu S. Combined treatment with endovenous laser ablation and compression therapy of incompetent perforating veins for treatment of recalcitrant venous ulcers. Phlebology. 2017 Jun;32(5):307-315. doi: 10.1177/0268355515594075. Epub 2015 Jun 30. PMID: 26130052.
Uthoff H, Keo HH, Spinedi L, Staub D. Perforator vein endovenous heat-induced thrombosis after laser ablation of the great saphenous vein. Vasa. 2020 Jun;49(4):330-332. doi: 10.1024/0301-1526/a000837. Epub 2019 Dec 6. PMID: 31808378.
Weber J. et May R.: Funktionelle Phlebologie: Georg Thieme Verlag Stuttgart; 1990; S.349 – 358
Winokur RS, Khilnani NM, Min RJ. Recurrence patterns after endovenous laser treatment of saphenous vein reflux. Phlebology. 2016 Aug;31(7):496-500. doi: 10.1177/0268355515596288. Epub 2015 Jul 16. PMID: 26187945.
https://www.thieme-connect.com/products/ejournals/pdf/10.12687/phleb2442-5-2018.pdf