
Saphenion® – Varicose veins in children/adolescents – What is useful, what is recommended?
Dr U Th Zierau; Saphenion® Vein Care Center Berlin / Rostock
Key words:
Varicose veins in children/adolescent; varicose veins in children, varicose veins in adolescents, endo-venous therapy of varicose veins, therapy indications, therapy recommendation
Saphenion® – Varicose veins in children/adolescents: Abstract
In the past, varicose vein therapy was practised with great caution in children and adolescents. The well-known radical surgical „ stripping “; pulling out the truncal varicose veins and side branches was in the imagination of the vascular surgeons really not suitable for working on the legs of young people – unless there was an acutely life-threatening finding (thrombosis) or a malformation (vascular tumour).


Saphenion® – Varicose veins in children/adolescents: Introduction
The tendency to varicose veins is already innate in over 90% of our patients. So, it is not the defective venous valve that turns the vein into a varicose vein, it is the defective vein wall that leads to the expansion of the cutaneous veins and thus sooner or later to the defective venous valve and thus to the development of the varicose veins. Young people are also affected to some extent. The congenital lack of venous valves, which is also possible, is a very rare exception.
In the literature, we find a large number of different information on the risk of developing varicose veins with a known family history. Positive family history is more common in boys and young men (80%) as well as in girls and young women (95%) with varicose veins than in both sexes without a positive family history. It is now certain that there is a hereditary component for varicose veins, but this is not solely responsible for the development of varicose veins. The already known risk factors also apply to adolescents. Intense competitive sport, long-standing, long sitting, excessive weight, hormone therapy, and the increased hormone release (Estrogen) in girls and young women play an essential role (1, 3, 4, 5, 7, 12, 15).
In the 32 years of my surgical – / vascular surgery activity since 1988, I have only performed a classic radical varicose vein operation on 4 young people. This is a negligible part of a total of 14,000 „ stripping “-operations. Regardless of this, there is of course an indication for therapy for truncal varicose veins of young people – because these have a chronically destructive effect on the entire leg vein system at an early stage. This is especially true for young girls and women shortly before and after menstruation – the regular release of estrogen hormones massively promotes vein dilation in the leg.
In our daily practice, we often experience that our patients receiving therapy – mothers and fathers – also ask about the risk for their own children in an educational talk. There is already a great deal of sensitivity to the disease „ varicose veins “, in general and the familial genesis and transmission of the risk to be recognized.
We recommend a duplex ultrasound examination of the pelvic and leg veins if there are no visual signs of the disease in the adolescent. This is painless, uncomplicated, and does not require any significant preparation. The only condition, however, is the presence of a parent in order to be able to discuss any visible pathological change diagnostically and therapeutically.
Saphenion® – Varicose veins in children/adolescents – our actual cases
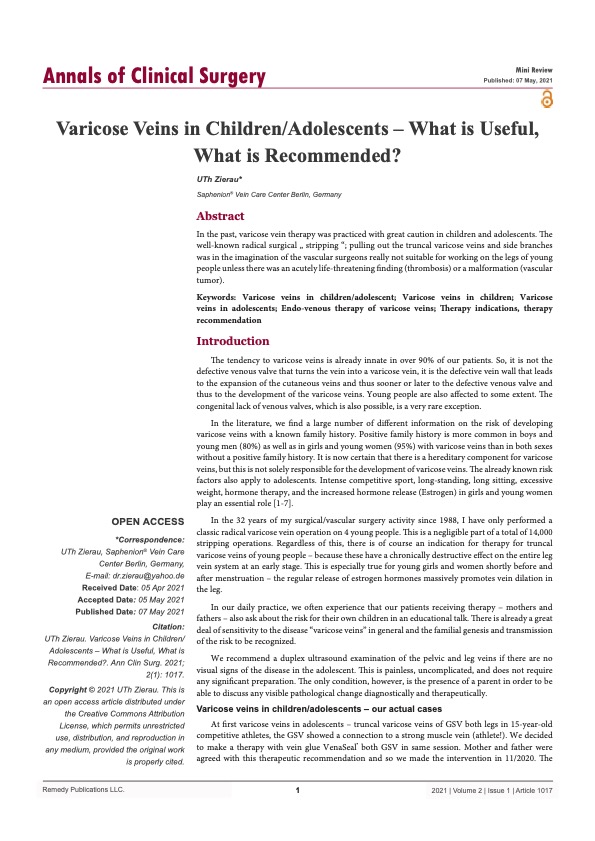
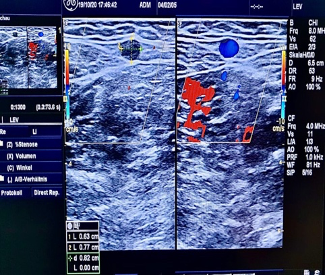
At first varicose veins in adolescents – truncal varicose veins of GSV both legs in 15-year-old competitive athletes, the GSV showed a connection to a strong muscle vein (athlete!). We decided to make therapy with vein glue VenaSeal® both GSV in the same session. The mother and father were agreed with this therapeutic recommendation and so we made the intervention on 11/2020. The vein diameter was in maximum of 0.8 cm and the duplex examination showed the typical pictures of backflow (Fig.1), (1, 3, 12, 15, 17).


The young patient gave us an impressive account of his symptoms and the impairments of being able to do his sport (basketball) in a competitive way. Two days after the treatment with the vein glue he began with jogging and gymnastics again (Fig.2), (1, 2, 12, 15).



Another very interesting case is a 5 years old boy. His mother came with him in our praxis in March 2021, and after the clinical examination and the colour duplex ultrasound we were very surprised and impressed – the 5 – year old boy had already developed lateral side branches and perforator varicose veins. However, he had no complaints yet, for him it was only a visible phenomenon at first. The mother also burdened with cramps, asked about an effective therapy (Fig.3) (1, 2, 3, 4, 12, 15).
The ultrasound examination of the truncal saphenous veins, however, was still normal, and there were no varicose truncal veins.


In the specialist team, we decided to wait and see; we asked the little boy’s somewhat impatient mother to be a little more patient. A re-presentation was agreed for the end of 2021. We explained the therapeutic options to the mother about Sealing Foam Therapy, a therapy using sealing micro-foam for the side branches and the perforator veins (1, 2, 15).
Saphenion® – Varicose veins in children/adolescents: Our discussion:
Since the year 2000, catheter-based procedures have been introduced into the therapy of truncal varicose veins – micro-foam, radio-waves, lasers, superheated steam, vein glue. Long-term results are now available – the radio-wave and the vein glue have also been proven to be effective in large-calibre veins > 1.5 cm in diameter. There is no longer any need to exercise restraint with the young patient. No longer a reason to practice a medically senseless wait-and-see attitude with the proven varicose vein because of radical surgical techniques. This no longer heals, not with cream, gel or tablet and not even with compression stockings (1, 2, 8, 10, 12, 13, 15)!
On the contrary, catheter procedures offer considerable advantages, especially for the young patient group, when one thinks of the side effects and complications of radical surgical techniques. And fully thought of the end of the therapy options, the cold non-thermal methods vein glue and micro-foam are the best for the therapy of young patients. No anaesthesia, no extensive tumescence anaesthesia – injections and with the VenaSeal® vein the young patient don`t need any more compression stockings. And we achieve immediate mobility for the adolescent patient (1, 2, 8, 10, 13, 14).
However, we take a critical view of the therapy recommendation of some colleagues to want to be active even with cosmetically disturbing network veins and spider veins on the young leg and to actively promote this. Here, a wait-and-see attitude continues until the pregnancies – because these cosmetically disruptive findings are largely hormone-induced. One – puncture therapy using micro-foam or the synonymous ScleroGlue “, on a visible network vein will then have to be repeated every 1 – 2 years and the findings escalate with existing hormone therapy (anti-baby pill) or pregnancy (8).
Finally, it should also be pointed out that the statutory health insurance companies have so far not created any possibility of gently and minimally invasive therapy for adolescents using catheter therapy. Even radical surgical therapy is usually not billable up to the age of 18 and remains a private service in Germany.
The author haven`t any conflict of interests.

Photos: Utzius, Nora
Papers / Links:
- Lambert G, Teplisky D, Cabezas M, Szhafir I, Silva M, Garriga M, Oliva A, Sierre S. Mechanochemical Endovenous Ablation of Varicose Veins in Pediatric Patients with Klippel-Trénaunay Syndrome: Feasibility, Safety, and Initial Results. J Vasc Interv Radiol. 2021 Jan;32(1):80-86. doi: 10.1016/j.jvir.2020.08.019. Epub 2020 Nov 1. PMID: 33139184.
- Redondo P, Bastarrika G, Sierra A, Martínez-Cuesta A, Cabrera J. Efficacy and safety of microfoam sclerotherapy in a patient with Klippel-Trenaunay syndrome and a patent foramen ovale. Arch Dermatol. 2009 Oct;145(10):1147-51. doi: 10.1001/archdermatol.2009.210. PMID: 19841402.
- Studennikova VV, Severgina LO, Dzyundzya AN, Korovin IA. Mekhanizmy razvitiia i osobennosti varikoznoĭ bolezni ven nizhnikh konechnosteĭ v detskom i molodom vozraste [Lower extremity varicose veins in childhood and at a young age: Mechanism of development and specific features]. Arkh Patol. 2017;79(4):56-60. Russian. doi: 10.17116/patol201779456-60. PMID: 28792000.
- Studennikova VV, Severgina LO, Korovin IA, Rapoport LM, Krupinov GE, Novikov IA. Ul’trastrukturnaya kharakteristika mekhanizmov varikoznoi transformatsii ven razlichnoi lokalizatsii [Ultrastructural characteristics of the mechanisms of varicose transformation of veins of different localization]. Arkh Patol. 2020;82(6):16-23. Russian. doi: 10.17116/patol20208206116. PMID: 33274621.
- https://www.saphenion.de/news/saphenion-krampfadertherapie-bei-kindern-jugendlichen/
Author`s address:
Dr. Ulf Th. Zierau, Friedrichstrasse 95, 10117 Berlin, Germany